

Lymphatic malformations are benign congenital malformations of the lymphatic system that occur predominantly in children. Most lymphatic malformations occur in the head and neck region, with those in abdominal locations, such as the mesentery, omentum and retroperitoneum, being less common, accounting for fewer than 5% of lymphatic malformations in children. This study analyzed the clinicopathologic characteristics and treatment outcomes of abdominal lymphatic malformations in children.
The medical records of 12 pediatric patients treated for abdominal lymphatic malformations at our institution between April 1999 and September 2017 were retrospectively reviewed. Demographic and clinical characteristics, including gender, age, symptoms and signs, diagnostic modalities, and treatment results, were analyzed.
The 12 patients included 11 boys and 1 girl, ranging in age from 3 months to 17 years (median 36.5 months) at presentation. The primary signs and symptoms included abdominal pain, abdominal mass and abdominal distention. Other symptoms and signs included fever, vomiting, scrotal pain and mass, and right inguinal mass. All patients were diagnosed by abdominal ultrasonography and computed tomography, and all underwent surgical excision with or without bowel resection. The lymphatic malformations occurred in the retroperitoneum (n=4), omentum (n=4), jejunal mesentery (n=2), and retroperitoneum and mesentery (n=2). Seven patients underwent complete mass excision, including 3 who underwent laparoscopic excisions, and 3 who underwent mass excision with segmental resection of the adjoining bowel. Two patients underwent incomplete excision because the lesion was extensive and invaded the superior mesenteric vessels. There was no major perioperative morbidity in any patient. At a median follow-up of 50 months (range, 8–183 months), only 1 patient experienced recurrence.
Although abdominal lymphatic malformations are benign, most children present with acute abdominal symptoms, necessitating early surgical treatment.
Citations
There have been a few reports of familial anorectal malformations extending over more than one generation. We experienced a case of a family with 3 members spanning 2 generations affected with isolated low type anorectal malformations. They had same low type of anorectal malformations. In all 3 patients, a perianal anoplasty was performed.
Median raphe cyst (MRC) of the perineum is rare congenital midline cyst of the male genitalia. MRC is thought to be caused by congenital alterations in the embryologic development of the male genitalia during fetal life. MRC can be found on the midline position between the urethral meatus and the anus. The lesion can be cystic, but sometimes it looks like an elongated configuration called a raphe canal. Diagnosis in childhood is particularly rare because they are usually asymptomatic, but some cases have reportedly been identified after infection. Although conservative treatment can be possible in small asymptomatic lesions, the treatment of choice is simple excision followed by primary closure in symptomatic cases. We describe here the case of 2-year-old boy presented at our institution with a 10-month history of anomaly of the perineal median raphe, which was treated by surgical excision.
The aim of this study was to identify the risk factor related to the need for operative treatment and avoid unnecessary non-operative management for intussusception in children. We retrospectively reviewed medical records of patient treated for intussusception at our institution between January 2006 and January 2013. Clinical features such as gender, age, seasonal variation, symptoms and signs, treatment results were analyzed. Univariate and multivariate analyses including a chi-square test for categorical variables and logistic regression analysis were performed. During the study period, 356 patients were treated for intussusception. 328 (92.1%) was treated successfully by the non-operative pneumoreduction, and 28 (7.9%) required operative management. On univariate analysis, risk factors which were related to the need for operative treatment were age, vomiting, bloody stool, lethargy, and symptoms duration. A logistic regression analysis in order to assess for independent predictors of operative treatment was performed. Age (<6 vs ≥12 months) (OR 4.713, 95% CI 1.198~18.539,
Citations
Congenital segmental dilatation of the colon is a very rare entity of unknown etiology, characterized by a localized dilatation of a bowel segment of the colon of variable length and an abrupt transition between the normal and dilated intestine. It can affect any part of the colon, with the rectosigmoid colon being the most commonly affected site. The clinical and radiological features may resemble that of Hirschsprung disease, but differ in that the normal ganglion cells are found in the dilated and normal segment of the colon. We performed laparoscopic-assisted transanal endorectal pull-through for segmental dilatation of rectosigmoid colon in an 8-year-old boy with chronic constipation since the age of 5 months.
Although hemangiomas are common vascular tumors that can occurany where in the body, they seldom involve the gastrointestinal tract. Hemangiomas of the gastrointestinal tract in infants and children are rare benign vascular tumors that most commonly present with gastrointestinal bleeding. We describe here the case of 2-year-old boy with intestinal bleeding caused by a large jejunal cavernous hemangioma, which was treated by laparoscopy-assisted resection of the affected portion of the jejunum.
Thyroglossal duct cysts (TGDC) are the most common type of congenital developmental anomaly encountered in the anterior midline of the neck in childhood. The aim of the study was to evaluate the clinical characteristics of TGDC and identify any factors that could be related to recurrence after surgery. This study consisted of a retrospective chart review of 45 patients treated at Kyungpook National University Hospital for TGDC between 1990 and 2008. All records were reviewed for age and sex, length of history, presentation, diagnostic methods, sizes and locations of cyst, surgical management, histopathology of the lesion and recurrences. The statistical analysis of risk factors for recurrence was made using the Fisher's exact test with a significance level of p < 0.05. The male to female ratio was 2.2:1 with a male preponderance. The mean age at operation was 5 years and 2 months (4 months – 17 years). The most common presenting symptom was a nontender cervical mass (78%). Most TGDC were found in the midline position. Twenty four were infrahyoid, 17 were hyoid, and 4 were suprahyoid level. Forty one (91%) patients received the Sistrunk operation, and 4(9%) patients received cyst excision. Postoperative a seroma developed in six patients in the early postoperative days. There were a total of 3(6.6%) recurrences, 2 in patients who had excision only and in one patient who had the Sistrunk operation. Univariate analysis for risk factors with recurrence showed that there was no statistical relationship between the presence of preoperative infection and the development of recurrence. The removal of hyoid bone along with TGDC was a statistically significant risk factor for recurrent disease. This study suggests that the Sistrunk operation is the treatment of choice for TGDC in order to reduce recurrence.
Gastric trichobezoars are commonly observed in young women with trichotillomania and trichophagia. We encountered an 8-year-old girl who had trichotillomania and trichophagia with abdominal pain and a mass, which was diagnosed as a large gastric trichobezoar. On physical examination, a huge, firm nontender mobile mass was palpated in her epigastrium. An upper gastrointestinal series and abdominal computed tomography (CT) scan showed a large mass in the stomach. Endoscopic removal was tried but failed. Laparoscopic removal was therefore performed. The trichobezoar was successfully retrieved through a gastrotomy and removed through an extended umbilical trocar incision. This case demonstrates that laparoscopic removal of large gastric trichobezoars is feasible and safe without a large abdominal incision.
Citations
We report a case of nonfunctioning neuroendocrine tumor of the pancreas in a 15-year-old girl who presented with back pain. On physical examination, there was mild tenderness in the left upper quadrant of the abdomen. The patient had no pancreatic hormone-associated symptoms. An abdominal ultrasonography showed a well-demarcated hypervascular solid mass with calcification in the tail of the pancreas. An abdominal computed tomography scan showed a 6x5cm sized well-encapsulated enhancing solid mass with cystic component in the tail of the pancreas. Distal pancreatectomy was performed. Pathology revealed awell- differentiated nonfunctioning low grade malignant neuroendocrine tumor of the pancreas. The postoperative course was uneventful.
Sertoli-Leydig cell tumor is a rare sex-cord stromal tumor of the ovary. They make up less than 0.5 % of all ovarian tumors. We experienced a case of an ovarian Sertoli-Leydig cell tumor in a 4 year-old girl who presented with nausea, vomiting, and lower abdominal pain of 2 days' duration. On physical examination, there was mild tenderness in the right lower quadrant of the abdomen. Abdominal ultrasonography and computed tomography (CT) scan revealed a pelvic mass measuring 5 × 3 cm that appeared to arise from the right ovary. At exploratory laparotomy, a 6 × 5 × 3 cm solid right ovarian mass without torsion was found. A right salpingo-oophorectomy was performed. The postoperative course was uneventful. The child was discharged 5 days after surgery.
Citations
Situs inversus abdominis is a rare congenital condition commonly associated with serious cardiac and splenic malformations. The importance of recognizing the presence of situs inversus abdominis preoperatively is emphasized by the fact that the surgical incision is placed on the incorrect side of the abdomen. A 6 day-old girl was referred to our hospital because of bile stained vomiting. A plain radiography of abdomen and chest showed the heart to be normal position and a reversed "double-bubble" picture with no other gas shadow in the rest of the abdomen. Abdominal computed tomography scan revealed situs inversus with the stomach and polysplenia on the right side and the liver on the left side. A laparotomy confirmed the diagnosis of situs inversus with duodenal atresia. The obstruction was bypassed by constructing a side-to-side duodenoduodenostomy. The postoperative course was uneventful.
Citations
Wandering spleen is very rare condition in children characterized by migration of the spleen from its normal position due to laxity or absence of the supporting splenic ligaments. We experienced a case of splenic infarction due to torsion of a wandering spleen in a 6-year-old boy who presented with fever, vomiting, and abdominal pain of 2 day's duration. On physical examination, there was severe tenderness in the left upper quadrant of the abdomen. The plain abdominal radiograph showed marked colonic gaseous distension. Contrast-enhanced abdominal computed tomography scan showed decreased density of spleen in the normal position, consistent with infarction. At emergency laparotomy, a wandering spleen twisted 360° on its pedicle was found. Despite splenic detorsion, blood flow could not be restored. Splenectomy was therefore performed. The child was discharged 7 days after surgery without any complications.
Citations
A 3-year-old boy with purulent otitis media received a chest radiograph as the part of a routine work up. The patient was normal appearing, in no acute distress. The patient's lung and heart sounds were clear and normal. The patient's abdomen was soft, non-distended, and non-tender. An anterior cardiophrenic mass was incidentally identified on the lateral chest radiograph. A computed tomography scan demonstrated a diaphragmatic hernia with bowel loops in the retrosternal space. An exploratory operation revealed a diaphragmatic defect (4 cm in diameter) on the left side of the falciform ligament, through which transverse colon was protruded. There was no hernia sac, and the defect was closed with interrupted No. 2 silk sutures. The child was discharged on the 8th postoperative day without any complications. During 6 months of follow-up period, recurrence was not noticed.
Four children with solid and papillary epithelial neoplasm of the pancreas are reported. Three were girls. Mean age at operation was 12 years and 7 months (10-13 years). Clinical presentation included nausea, vomiting, and apalpable mass. One had hemoperitoneum due to tumor rupture. In two cases, tumors were in the body of the pancreas, and one the body and tail, and in one,the tail. Mean diameter of the tumors was 10.8 cm (8-15cm). Surgical procedures were distal pancreatectomy and splenectomy in 2 cases, distal pancreatectomy in one, and subtotal pancreatectomy and splenectomy in one. Mean follow-up period was 61 months (6-121 months). Three patients are still alive without any recurrence. However, in the one case of ruptured tumor, portal vein thrombosis and liver metastasis developed after subtotal pancreatectomy and splenectomy during the course of postoperative adjuvant chemotherapy.
A 10-year-old-girl who underwent Roux-en-Y cystojejunostomy under the diagnosis of choledochal cyst at another hospital at the age of 3 months was referred to our hospital due to abdominal pain. Abdominal ultrasonography (USG) and computed tomography (CT) showed the type I choledochal cyst and multiple gall bladder stones. Severe inflammation and adhesion made difficulty of radical resection and only partial resection of choledochal cyst with Roux-en-Y hepaticojejunostomy could be performed. She complained of intermittent abdominal pain, fever, nausea and vomiting 2 1/2 years after the second operation. Follow-up abdominal CT scan showed the polypoid nodular lesion in the remnant choledochal cyst and suspicious metastatic lesion in the segment 7 of the liver. The duodenum was obstructed by the mass arising from the remnant choledochal cyst. The USG-guided liver biopsy revealed the moderately differentiated adenocarcinoma. A secondary palliative gastrojejunostomy was performed to relieve the obstruction of duodenum. She died of hepatic insufficiency 4 months later of third operation.
An 11-year-old girl with history of two previous attacks of acute pancreatitis was admitted to another hospital. On physical examination, she had epigastric tenderness. Laboratory studies included amylase of 657IU/L and lipase of 3131IU/L. Abdominal computed tomography (CT) scan suggested necrosis in 30% of pancreas. To establish the cause of recurrent pancreatitis, endoscopic retrograde cholangiopancreatography (ERCP) was performed after acute pancreatitis subsided. Duodenoscopic view revealed a blind sac covered by normal duodenal mucosa at the second portion of the duodenum. Barium upper gastrointestinal series (UGI) showed a large sac separated from adjacent duodenal lumen by a radiolucent band. Diagnosis of intraluminal duodenal diverticulum (IDD) was made and endoscopic excision was considered. The apex of the diverticulum was incised endoscopically using a needle knife papillotome. At a follow-up endoscopy one day after procedure, bleeding from the incised edge of diverticulum was noted. Despite hemoclipping and injection of hypertonic saline-epinephrine solution by under the endoscopy, hemostasis was unsuccessful. She was transferred to the Kyungpook National University Hospital after resuscitation. Open duodenotomy and excision of the diverticulum were performed. She has recovered well from surgery and remains asymptomatic.
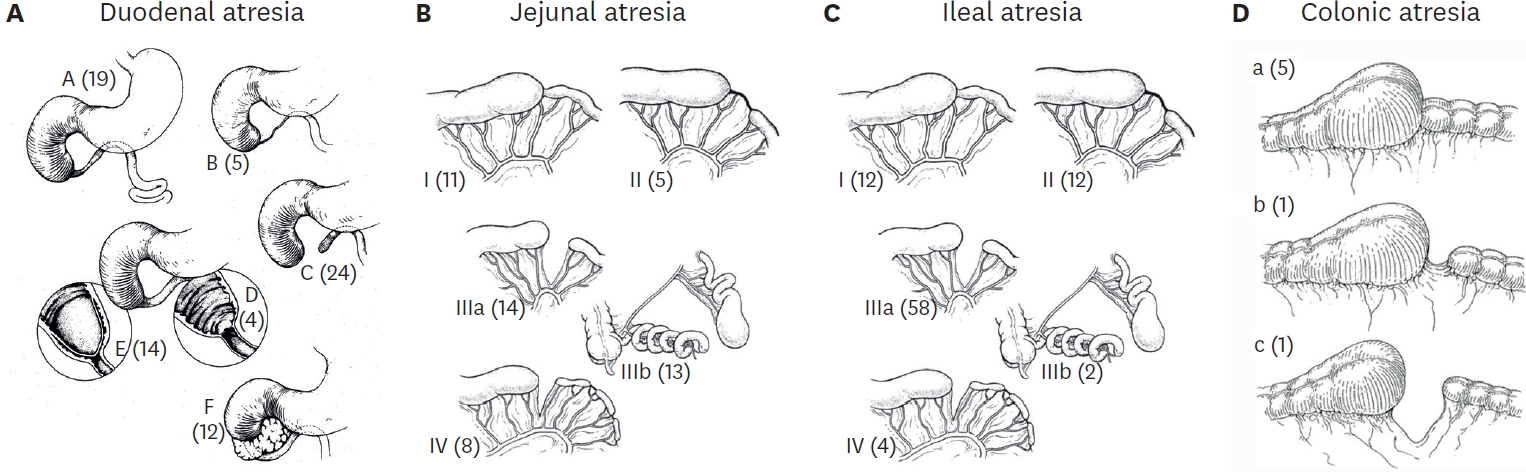
Intestinal atresia is a frequent cause of intestinal obstruction in the newborn. We reviewed the clinical presentation, associated anomalies, types of atresias, operative managements, and early postoperative complications in 36 cases of intestinal atresia treated at the Department of Surgery, Kyungpook National University Hospital between January 1994 and February 2003. Location of the lesion was duodenum in 17 patients, jejunum in 11 patients and ileum in 8 patients. The male to female ratio was 1:1.4 in duodenal atresia (DA), 2.7:1 in jejunal atresia (JA) and 7:1 in ileal atresia (IA). The most common type was type III (41.1 %) in DA, and type I (52.6 %) in JA and IA. The most common presenting symptoms was vomiting(88.2 %) in DA, but in jejunoileal atresia, vomiting(89.4 %) and abdominal distension(89.4 %) were the most common sign and symptom. All cases of DA were diagnosed by plain abdominal radiography. There were 6 cases of DA with congenital heart disease, 3 cases of DA with Down syndrome and 3 cases of JA with meconium peritonitis. Segmental resection was performed in 13 cases, duodenoduodenostomy in 11 cases, membrane excision in 7 cases, jejunojejunostomy in 2 cases, gastroduodenostomy in 2 cases and ileocolic anastomosis in 1 case. There were 9 postoperative complications including 3 each of anastomotic leakage, wound infection, and intestinal obstruction 3 cases. The mortality rate for DA was 11.8 %(2/17). Both deaths in DA were attributed to congenital heart disease. The mortality rate for JA was 18% (2/11). Both cases died with sepsis and short bowel syndrome.
Citations
Spontaneous gastric perforation in the newborn is a rare disease that requires early diagnosis and prompt surgical treatment. Between 1988 and 2001 at the Department of Pediatric Surgery, Kyungpook National University Hospital, 9 cases of spontaneous gastric perforation were treated. Seven were males and two females. The mean gestational age and birth weight were 36.7 weeks and 2,455 grespectively. All patients presented with severe abdominal distention and pneumoperitoneum on cross table lateral film of the abdomen. Perforations were located on the anterior wall along the greater curvature of the stomach in six and on the posterior wall along the greater curvature in two. One case showed two sites of perforation on the anterior and posterior wall along the greater curvature. Six patients were managed with debridement and primary closure and the others with debridement and partial gastrectomy. Peritoneal drainage was not performed. There were four deaths; two from sepsis due to leakage from the anastomotic site, one as a result of acute renal failure, and the other by associated respiratory distress syndrome. Spontaneous gastric perforation in the newborn is usually located along the greater curvature. Elevated intragastric pressure is a possible cause of the perforation. Poor prognosis is related to associated diseases and prematurity.
Citations
Between March 1999 and January 2000, 82 boys with the diagnosis of inguinal hernias (12 bilateral and 70 unilateral hernias), underwent Ultrasound (US) examination of both sides of the groin, a total of 164 inguinal imaging prior to surgery. The patients ages ranged from 3 days to 12 years with a mean of 32.6 months. Ninty four examinations were on the clinically symptomatic side and 70 were on the asymptomatic side. The US criteria for the diagnosis of an inguinal hernia were as follows: 1) visceral hernia, the presence of bowel loops, or omentum in the inguinal canal, 2) communicating hydrocele, the presence of fluid in the processus vaginalis, 3) widening of patent processus vaginalis at the level of nternal inguinal ring. The width of patent processus vaginalis at the level of internal inguinal ring over 4 mm is onsidered an occult hernia. Among the 94 symptomatic groins, US findings showed 31 (33 %) visceral hernias, 18 (19 %) communicating hydroceles, and 38 (41 %) widening of the internal inguinal ring, and 7 (7 %) groins without abnormalities. In 70 asymptomatic groins, there were 4 (6 %) visceral hernias, 5 (7 %) communicating hydroceles, 11 (16 %) widening of the internal inguinal ring, and 50 (70 %) groins without abnormalities. Among the 70 asymptomatic groins there were US abnormalities in 20 (28 %). One hundred and seven groins with positive US findings were surgically explored. Among 107 operated sites, the operative findings were compatible with the US diagnosis in 104, a sensitivity for US of 97.2 %. In patients with US findings of widening of internal inguinal ring (>4 mm), there was patent processus vaginalis in 36 out of 38 symptomatic groins and 10 of 11 asymptomatic groins. The sensitivity of US to the operative findings in widening of internal inguinal ring was 93.8 %. For visceral hernia and communicating hydrocele, the sensitivity of positive US findings was 100 %. Ultrasonography for inguinal hernias appears to be a rapid, reliable, and noninvasive screening diagnostic tool with high positive specificity. Therefore, we recommend the use of US as a routine diagnostic tool in pediatric patients with inguinal hernias and hydroceles.
Citations
 First
First Prev
Prev

