ABSTRACT
-
Purpose
At our institution, congenital duodenal atresia is repaired laparoscopically using duodenoduodenostomy with a parallel anastomosis. During our use of this technique, we noted that after mobilization, the distal duodenal segment naturally rested in either a cranial or caudal orientation relative to the proximal segment and that this resting orientation appeared to vary with the anatomical level of atresia. This study primarily evaluated the association between atresia location and the natural orientation of the distal duodenal segment. It secondarily compared perioperative outcomes between the cranial and caudal orientation groups.
-
Methods
This retrospective cohort study was conducted at Samsung Medical Center (Seoul, South Korea) and included neonates who underwent laparoscopic duodenoduodenostomy with parallel anastomosis for congenital duodenal atresia from January 2008 to June 2021. After patients with annular pancreas or duodenal web were excluded, 22 neonates were analyzed and categorized into the cranial (n=16) or caudal (n=6) orientation group according to intraoperative findings. Perioperative outcomes were compared, and the relationship between atresia location and distal segment orientation was analyzed.
-
Results
Operative time, postoperative ventilator support, time to feeding initiation, time to full feeding, and length of hospitalization did not differ significantly between groups. No patient required conversion to open surgery, developed an anastomotic stricture, or died during hospitalization. One patient in the cranial group developed an anastomotic leak, which was treated by laparoscopic reanastomosis. First-portion duodenal atresia was significantly more frequent in the caudal group than in the cranial group (83.3% vs. 25.0%, P=0.023).
-
Conclusion
Laparoscopic duodenoduodenostomy with parallel anastomosis was feasible in both cranial and caudal orientations, with no conversions to open surgery. The natural orientation of the distal duodenal segment was significantly associated with the anatomical location of atresia, supporting an anatomical basis for orientation-guided parallel anastomosis.
-
Keywords: Duodenal atresia; Duodenoduodenostomy; Laparoscopy; Infant
INTRODUCTION
Duodenal atresia is a congenital intestinal obstruction that occurs in approximately 1 in 5,000–10,000 live births and is often accompanied by trisomy 21, congenital heart defects, or other gastrointestinal malformations [
1,
2]. Duodenoduodenostomy is the definitive operative treatment, and current long-term survival rates exceed 90% [
3,
4]. Even with these favorable survival outcomes, technical aspects of reconstruction remain clinically relevant because they can contribute to postoperative complications such as anastomotic leak, stricture, and delayed enteral feeding [
4,
5].
Over the past two decades, laparoscopic duodenoduodenostomy has become an accepted minimally invasive approach in specialized pediatric surgical centers, where it can reduce surgical trauma, improve operative visualization, and support faster recovery [
6-
9]. The diamond-shaped anastomosis introduced by Kimura et al. [
10] remains the most widely used configuration [
11-
13]. Our institution uses a parallel anastomosis technique in which the proximal and distal duodenal segments are approximated according to their natural alignment rather than rotated into a predetermined configuration [
14]. As our experience with this approach increased, we observed that the distal duodenal segment rested in one of two reproducible orientations—cranial or caudal—relative to the proximal segment and that this orientation appeared to correspond to the anatomical location of the atresia [
15,
16].
Although laparoscopic repair of duodenal atresia has been increasingly reported, few studies have examined how the level of atresia relates to the intraoperative alignment of the duodenal segments or to the selected anastomotic configuration [
8,
17,
18]. The primary aim of this study was therefore to characterize the association between duodenal atresia location and the natural orientation of the distal duodenal segment during laparoscopic parallel anastomosis. The secondary aim was to compare perioperative outcomes between the cranial and caudal orientation groups as an assessment of the feasibility of this anatomy-guided approach.
METHODS
Ethics statement
This single-center retrospective cohort study was approved by the Institutional Review Board of Samsung Medical Center (No. 2024-12-137). The requirement for informed consent was waived because the study used a retrospective design.
Study design and patient selection
We reviewed all neonates who underwent laparoscopic duodenoduodenostomy for congenital duodenal atresia between January 2008 and June 2021. Among 29 initially identified patients, seven were excluded after intraoperative findings showed annular pancreas or duodenal web. Patients with duodenal atresia accompanied by annular pancreas were excluded because an encircling pancreatic ring may independently change the spatial relationship between the proximal and distal duodenal segments, thereby confounding assessment of their natural orientation. Patients with duodenal web were excluded because this obstruction differs mechanistically from true atresia. The final study cohort comprised 22 neonates (
Fig. 1).
The operative technique followed our previously published protocol [
14]. Two experienced pediatric surgeons performed all procedures. A four-trocar configuration was used, consisting of a 5-mm transumbilical camera port, two 3-mm working ports placed on either side of the umbilicus, and a 3-mm epigastric assistant port. After the duodenal C-loop had been mobilized, the distal duodenal segment was allowed to settle into its natural perpendicular relationship to the proximal segment without forced rotation. A transverse incision was made in the proximal duodenum, and a longitudinal incision was made in the distal duodenum to create parallel openings. The anastomosis was constructed posterior wall first with interrupted 5-0 glyconate monofilament absorbable sutures (Monosyn, B. Braun). An orogastric tube was routinely placed for gastric decompression in all patients.
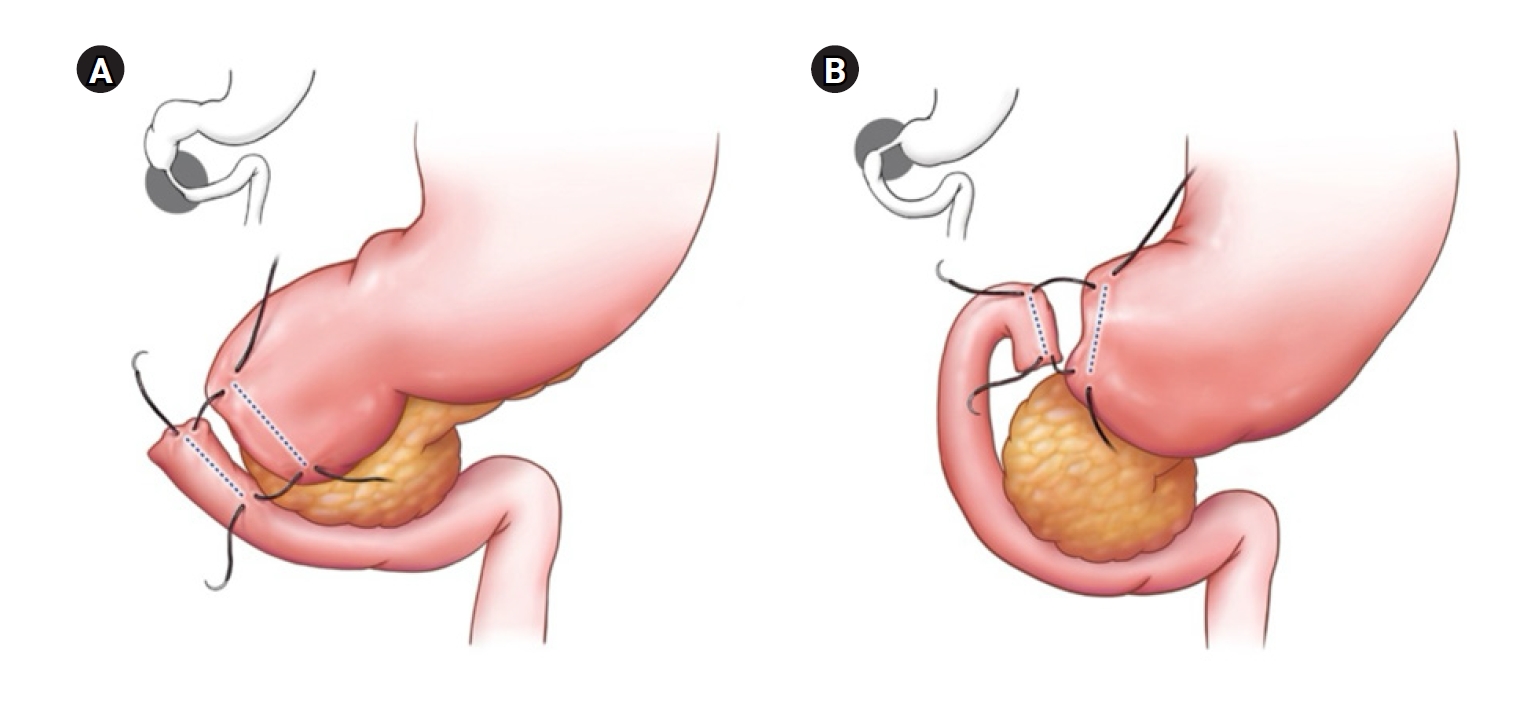
The distal segment was classified as having a cranial orientation when it was directed toward the head and as having a caudal orientation when it was directed toward the feet, based on its resting position after mobilization (
Fig. 2). Orientation was determined after Kocherization and mobilization of the duodenal C-loop and before stay sutures were placed. The classification relied on the unforced resting position of the distal segment relative to the proximal segment, with no traction applied. This orientation was documented in the operative notes at the time of surgery and later confirmed by review of the operative video recordings. In every case, the orientation could be classified clearly, and no intermediate or borderline orientation was encountered.
Atresia location was assigned according to intraoperative anatomical landmarks. First-portion atresia was defined as obstruction proximal to the expected ampullary region and was identified by the absence of bile staining in the proximal duodenal lumen together with the relationship between the atretic segment and the pancreatic head. Postampullary atresia was defined as obstruction at or distal to the expected ampullary level and was typically recognized by bile-stained fluid in the proximal segment.
Data collection
The collected variables included demographic characteristics, associated anomalies, atresia location, operative time, duration of postoperative ventilator support, time to feeding initiation, time to full feeding, length of hospitalization, and complications. Enteral feeding was started after nasogastric output had decreased to less than 5 mL/kg/day and radiographic passage of intestinal gas had been confirmed.
Statistical analysis
A formal sample-size calculation was not performed because the retrospective cohort included all eligible patients treated during the study period. No data were missing for the primary variables included in the analysis.
Continuous variables were summarized as median (range) and compared with the Mann-Whitney U test. Categorical variables were compared with the Fisher exact test. Statistical significance was defined as P<0.05. All analyses were performed using IBM SPSS ver. 25 (IBM Corp.).
RESULTS
In total, 22 neonates underwent laparoscopic duodenoduodenostomy with parallel anastomosis; 16 were assigned to the cranial orientation group and six to the caudal orientation group. No procedure required conversion to open surgery. The cohort included 11 male neonates (50.0%). Median gestational age was 37+1 weeks (range, 35+3 to 38+6 weeks), and median birth weight was 2,575 g. The median age at surgery was 2.5 days, and median body weight at operation was 2,400 g. Associated anomalies were identified in seven patients (31.8%) and included Down syndrome (n=5), congenital heart defects (n=4), esophageal atresia (n=1), and limb anomalies (n=1). Gastrointestinal malrotation was found in one patient (4.5%) and was reported separately because it represented a distinct surgical finding that could influence intraoperative anatomy.
Table 1 summarizes the baseline characteristics according to orientation group. Gestational age, birth weight, and the presence of associated anomalies were not significantly different between groups. Male sex was more frequent in the caudal group than in the cranial group (83.3% vs. 37.5%), but this difference did not reach statistical significance (P=0.149).
Atresia location was significantly associated with the natural orientation of the distal duodenal segment. First-portion duodenal atresia occurred more often in the caudal group than in the cranial group (83.3% vs. 25.0%, P=0.023).
Table 2 presents perioperative outcomes. Body weight at operation (2,335 g vs. 2,695 g, P=0.073) and age at operation (3 days vs. 2 days, P=0.474) were not significantly different between groups. Median operative time was numerically shorter in the caudal group than in the cranial group (109 minutes [range, 95–147 minutes] vs. 134.5 minutes [range, 95–248 minutes]), but this difference was not statistically significant (P=0.186).
Short-term postoperative outcomes were similar between the cranial and caudal orientation groups. Duration of postoperative ventilator support (1 day [range, 0–13 days] vs. 1 day [range, 0–5 days], P=0.920), length of hospital stay (13.0 days [range, 9–107 days] vs. 12.5 days [range, 10–39 days], P=0.677), time to feeding initiation (5 days [range, 3–30] vs. 5 days [range, 3–9], P=0.755), and time to full feeding (10.0 days [range, 6–45 days] vs. 9.5 days [range, 7–15 days], P=0.679) did not differ significantly. Median follow-up duration also did not differ significantly between groups (6.6 months vs. 7.3 months, P=0.900).
Postoperative complications were recorded in one patient (6.3%) in the cranial group and in no patients in the caudal group (P>0.999). The affected patient developed an anastomotic leak that was successfully treated with laparoscopic reanastomosis. No anastomotic strictures were observed, and no in-hospital deaths occurred in either group.
DISCUSSION
In this retrospective cohort, perioperative outcomes after laparoscopic duodenoduodenostomy with parallel anastomosis showed no statistically significant differences between the cranial and caudal orientation groups. During the available follow-up period, no anastomotic strictures were identified, no in-hospital deaths occurred, and the single anastomotic leak was successfully treated by laparoscopic reanastomosis. The main statistically significant finding was the association between atresia location and distal segment orientation: first-portion atresia was predominantly associated with caudal orientation, whereas postampullary atresia was associated with cranial orientation (P=0.023). This association is the principal observation of this study and suggests that the natural alignment encountered during parallel anastomosis may reflect, at least in part, the anatomical level of obstruction. Because the cohort was small and had limited statistical power, the lack of significant between-group differences in perioperative outcomes should not be interpreted as evidence of equivalence.
The anatomical configuration of the duodenum provides a plausible explanation for this pattern. When atresia involves the first portion of the duodenum, the short proximal segment and its proximity to the pylorus may restrict cranial mobilization, allowing the distal segment to rest in a caudal position after mobilization. When atresia is postampullary, the longer proximal duodenal segment may permit the distal segment to be mobilized more readily in a cranial direction. Aligning the anastomosis with this natural orientation may reduce the need for forced rotation or excessive traction and may facilitate tension-free reconstruction [
14]. This anatomical rationale differentiates parallel anastomosis from techniques that depend on a predefined anastomotic configuration.
A wide, tension-free anastomosis is a central technical principle in surgery for duodenal atresia [
4,
10,
19]. Kimura et al. [
10] introduced the diamond-shaped anastomosis to increase the anastomotic lumen, and favorable long-term outcomes have been reported with this configuration [
3,
20]. Parallel anastomosis is designed to create a comparably wide opening while maintaining the natural orientation of the proximal and distal segments [
14]. Several series have supported the feasibility and safety of laparoscopic duodenoduodenostomy [
6,
7,
11,
21], and systematic reviews have reported outcomes comparable to those of open repair [
8,
22]. The present findings extend these reports by showing that orientation-based parallel anastomosis could be completed in both natural orientations without conversion to open surgery; however, the small sample size and limited follow-up prevent firm conclusions about comparative safety or long-term outcomes.
Previous studies have mainly compared laparoscopic with open repair [
9,
17,
22] or assessed outcomes according to anastomotic configuration [
12,
23]. In contrast, anastomotic orientation itself has rarely been examined as a separate anatomical variable. Jhala et al. [
18] evaluated whether anastomotic technique affected outcomes, but their analysis did not stratify patients by distal segment orientation or atresia location. The present study therefore focused on the natural orientation of the distal duodenal segment as observed intraoperatively during a single standardized procedure.
A distinctive feature of this study is that group assignment was determined by an intraoperative anatomical finding—the natural orientation of the distal duodenal segment—rather than by differences in operative technique. Because the same standardized procedure was used in both groups, technique-related variability was reduced, allowing perioperative outcomes to be described across two anatomical configurations encountered during the same operative approach. The groups nevertheless differed significantly in atresia location, which also formed the basis of the observed association. Accordingly, the outcome comparison should not be interpreted as isolating the effect of orientation alone, because unmeasured confounding related to atresia location cannot be excluded. Awareness of the relationship between atresia location and natural orientation may help surgeons anticipate the intraoperative configuration and select enterotomy sites and suture placement along the most natural, tension-free axis. Whether preserving this natural orientation directly improves anastomotic tension, surgical ergonomics, or postoperative function remains a hypothesis that should be examined in prospective studies. To our knowledge, this is the first study to systematically describe this relationship during laparoscopic parallel duodenoduodenostomy.
This study has several limitations. First, its retrospective design creates the possibility of selection and information bias. Second, the cohort was small, especially the caudal orientation group, which limited statistical power and generalizability. More detailed subclassification of atresia location (e.g., D1, D2, D3) was not feasible because the number of patients was limited and precise anatomical localization is difficult in neonatal duodenal atresia. Third, the study was conducted at a single center using a standardized institutional technique, so the findings may not be directly applicable to centers that use different operative strategies. Fourth, because no comparison group underwent diamond-shaped anastomosis, the relative advantages of parallel anastomosis could not be determined. Finally, follow-up was relatively short, which limited assessment of long-term anastomotic and functional outcomes. In particular, the minimum follow-up of 0.8 months in some patients was insufficient for evaluation of late complications such as anastomotic stricture or functional dysmotility; therefore, the reported complication rates should be interpreted in light of this limitation.
In conclusion, during laparoscopic orientation-based parallel anastomosis, the natural orientation of the distal duodenal segment was significantly associated with the anatomical location of duodenal atresia. The operation was completed in both cranial and caudal orientations, with no conversion to open surgery. Short-term perioperative outcomes did not differ significantly between the orientation groups, but these results should be interpreted cautiously because of the small sample size, limited follow-up, and lack of a conventional anastomosis control group. Larger studies with longer follow-up are needed to validate this anatomical association and determine its clinical relevance.
NOTES
-
Authors’ contributions
Conceptualization: MJB, WK, SL. Data curation: MJB, SJK. Formal analysis: SJK, WK. Investigation: WK, SP. Methodology: MJB, SL. Visualization: WK, SL. Writing–original draft: MJB, SJK, WK. Writing–review & editing: MJB, SL, JMS. All authors read and approved the final manuscript.
-
Conflict of interest
Sanghoon Lee is an editorial board member of this journal, but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Data availability
All data generated or analyzed during this study are included in this published article. For other data, these may be requested through the corresponding author.
Fig. 1.Flowchart of patient selection.
Fig. 2.Schematic illustration of parallel anastomosis according to the natural orientation of the distal duodenal segment during laparoscopic duodenoduodenostomy. (A) Cranial orientation of the distal duodenal segment. (B) Caudal orientation of the distal duodenal segment. Dotted lines indicate the planned enterotomy sites in the proximal and distal duodenal segments.
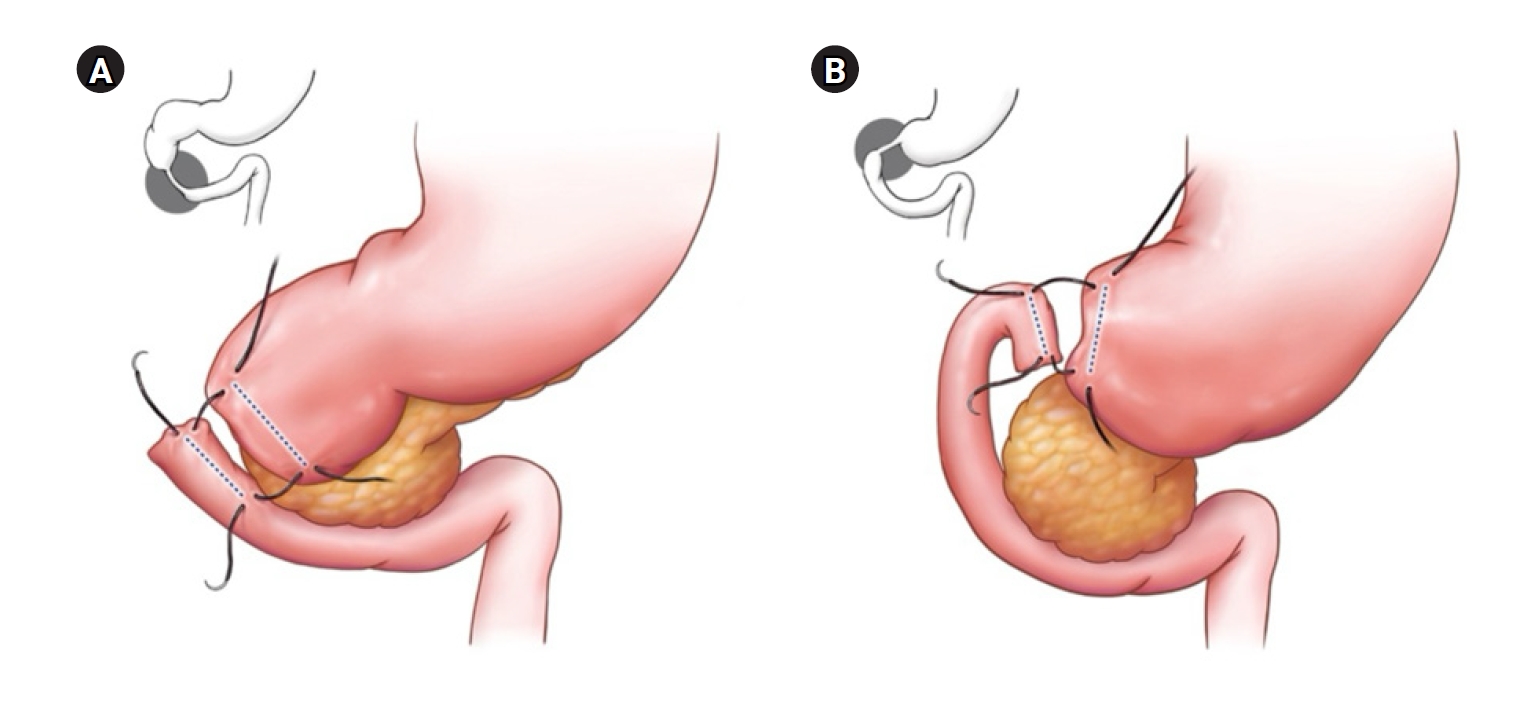
Table 1.Patients’ demographic and baseline characteristics between the cranial and caudal orientation groups
Table 1.
|
Characteristic |
Overall (n=22) |
Cranial group (n=16) |
Caudal group (n=6) |
P-value |
|
Male sex |
11 (50.0) |
6 (37.5) |
5 (83.3) |
0.149 |
|
Gestational age (wk+day) |
37+1 (35+3 to 38+6) |
37+1 (35+3 to 38+6) |
37+6 (36+5 to 38+4) |
0.079 |
|
Birth weight (g) |
2,575 (1,470–3,200) |
2,466 (1,470–3,200) |
2,840 (2,180–3,040) |
0.101 |
|
Associated anomalies |
7 (31.8) |
5 (31.3) |
2 (33.3) |
>0.999 |
|
Gastrointestinal malrotation |
1 (4.5) |
1 (6.3) |
0 (0) |
>0.999 |
|
First-portion duodenal atresia |
9 (40.9) |
4 (25.0) |
5 (83.3) |
0.023*
|
Table 2.Perioperative characteristics and outcomes between the cranial and caudal orientation groups
Table 2.
|
Characteristic |
Overall (n=22) |
Cranial group (n=16) |
Caudal group (n=6) |
P-value |
|
Body weight at operation (g) |
2,400 (1,410–3,100) |
2,335 (1,410–3,100) |
2,695 (2,180–2,880) |
0.073 |
|
Age at operation (day) |
2.5 (1–16) |
3.0 (1–16) |
2.0 (1–12) |
0.474 |
|
Operative time (min) |
134.0 (95–248) |
134.5 (95–248) |
109.0 (95–147) |
0.186 |
|
Postoperative ventilator day |
1 (0–13) |
1 (0–13) |
1 (0–5) |
0.920 |
|
Postoperative hospital day |
13.0 (9‒107) |
13.0 (9‒107) |
12.5 (10‒39) |
0.677 |
|
Time to initiation of feeding (day) |
5 (3‒30) |
5 (3‒30) |
5 (3‒9) |
0.755 |
|
Time to full feeding (day) |
10.0 (6‒45) |
10.0 (6‒45) |
9.5 (7‒15) |
0.679 |
|
Follow-up (mo) |
6.7 (0.8–71.7) |
6.6 (0.8–71.7) |
7.3 (0.9–59.0) |
0.900 |
|
Postoperative complication |
1 (4.5) |
1 (6.3)a)
|
0 (0) |
>0.999 |
|
Mortality during hospitalization |
0 (0) |
0 (0) |
0 (0) |
NA |
REFERENCES
- 1. Fonkalsrud EW, DeLorimier AA, Hays DM. Congenital atresia and stenosis of the duodenum: a review compiled from the members of the Surgical Section of the American Academy of Pediatrics. Pediatrics 1969;43:79-83.
- 2. Choudhry MS, Rahman N, Boyd P, Lakhoo K. Duodenal atresia: associated anomalies, prenatal diagnosis and outcome. Pediatr Surg Int 2009;25:727-30.
- 3. Escobar MA, Ladd AP, Grosfeld JL, et al. Duodenal atresia and stenosis: long-term follow-up over 30 years. J Pediatr Surg 2004;39:867-71.
- 4. Grosfeld JL, Rescorla FJ. Duodenal atresia and stenosis: reassessment of treatment and outcome based on antenatal diagnosis, pathologic variance, and long-term follow-up. World J Surg 1993;17:301-9.
- 5. Koenig SM, Russell RT, Quevedo OG, Chen MK. Intestinal atresias: a ten-year evaluation of outcomes. J Surg Res 2024;296:130-4.
- 6. Bax NM, Ure BM, van der Zee DC, van Tuijl I. Laparoscopic duodenoduodenostomy for duodenal atresia. Surg Endosc 2001;15:217.
- 7. Rothenberg SS. Laparoscopic duodenoduodenostomy for duodenal obstruction in infants and children. J Pediatr Surg 2002;37:1088-9.
- 8. Mentessidou A, Saxena AK. Laparoscopic repair of duodenal atresia: systematic review and meta-analysis. World J Surg 2017;41:2178-84.
- 9. Chung PH, Wong CW, Ip DK, Tam PK, Wong KK. Is laparoscopic surgery better than open surgery for the repair of congenital duodenal obstruction?: a review of the current evidences. J Pediatr Surg 2017;52:498-503.
- 10. Kimura K, Mukohara N, Nishijima E, Muraji T, Tsugawa C, Matsumoto Y. Diamond-shaped anastomosis for duodenal atresia: an experience with 44 patients over 15 years. J Pediatr Surg 1990;25:977-9.
- 11. van der Zee DC. Laparoscopic repair of duodenal atresia: revisited. World J Surg 2011;35:1781-4.
- 12. Parmentier B, Peycelon M, Muller CO, El Ghoneimi A, Bonnard A. Laparoscopic management of congenital duodenal atresia or stenosis: a single-center early experience. J Pediatr Surg 2015;50:1833-6.
- 13. Jung E, Son NH. Laparoscopic management of duodenal atresia: a decade of single surgeon’s perspective. Ann Surg Treat Res 2026;110:127-34.
- 14. Oh C, Lee S, Lee SK, Seo JM. Laparoscopic duodenoduodenostomy with parallel anastomosis for duodenal atresia. Surg Endosc 2017;31:2406-10.
- 15. Gharpure V. Duodenal atresia. J Neonatal Surg 2014;3:14.
- 16. Miscia ME, Lauriti G, Lelli Chiesa P, Zani A. Duodenal atresia and associated intestinal atresia. Pediatr Surg Int 2019;35:151-7.
- 17. Spilde TL, St Peter SD, Keckler SJ, Holcomb GW, Snyder CL, Ostlie DJ. Open vs laparoscopic repair of congenital duodenal obstructions: a concurrent series. J Pediatr Surg 2008;43:1002-5.
- 18. Jhala T, Aichner J, Berger L, et al. Minimal invasive duodenal atresia repair: does surgical technique of anastomosis matter? A systematic review and meta-analysis. J Pediatr Surg 2025;60:162493.
- 19. Chen QJ, Gao ZG, Tou JF, et al. Congenital duodenal obstruction in neonates: a decade's experience from one center. World J Pediatr 2014;10:238-44.
- 20. Piper HG, Alesbury J, Waterford SD, Zurakowski D, Jaksic T. Intestinal atresias: factors affecting clinical outcomes. J Pediatr Surg 2008;43:1244-8.
- 21. Valusek PA, Spilde TL, Tsao K, St Peter SD, Holcomb GW, Ostlie DJ. Laparoscopic duodenal atresia repair using surgical U-clips: a novel technique. Surg Endosc 2007;21:1023-4.
- 22. Zuccarello B, Spada A, Centorrino A, Turiaco N, Chirico MR, Parisi S. The modified Kimura’s technique for the treatment of duodenal atresia. Int J Pediatr 2009;2009:175963.
- 23. St Peter SD, Little DC, Barsness KA, et al. Should we be concerned about jejunoileal atresia during repair of duodenal atresia? J Laparoendosc Adv Surg Tech A 2010;20:773-5.