

Diverticular bleeding and gastric heterotopia (GHT) in the proximal lower gastrointestinal tract are rare in adolescents. Here, we report a case of cecal diverticular bleeding associated with GHT. A 17-year-old adolescent boy was discharged after treatment for cecal diverticular bleeding. Subsequently, he visited the hospital due to an episode of hematochezia and sustained pain in the right lower abdomen. A colon study showed a diverticulum causing external compression in the cecum. His hemoglobin level was 7.2 g/dL. Abdominopelvic computed tomography showed thickening of the ascending and transverse colon, suggesting non-specific colitis. Single-incision laparoscopic ileocecal resection was performed. Pathologic findings demonstrated congenital diverticulum with GHT in the cecum, and an ulcer with perforation in the cecal area. In cases of hematochezia among adolescents, clinicians should be aware of the possibility of rare diseases such as GHT.
Diverticular bleeding and gastric heterotopia (GHT) in the proximal lower gastrointestinal tract are rare in adolescents. Here, we report a case of cecal diverticular bleeding associated with GHT. A 17-year-old adolescent boy was discharged after treatment for cecal diverticular bleeding. Subsequently, he visited the hospital due to an episode of hematochezia and sustained pain in the right lower abdomen. A colon study showed a diverticulum causing external compression in the cecum. His hemoglobin level was 7.2 g/dL. Abdominopelvic computed tomography showed thickening of the ascending and transverse colon, suggesting non-specific colitis. Single-incision laparoscopic ileocecal resection was performed. Pathologic findings demonstrated congenital diverticulum with GHT in the cecum, and an ulcer with perforation in the cecal area. In cases of hematochezia among adolescents, clinicians should be aware of the possibility of rare diseases such as GHT.
Gastric heterotopia (GHT) is characterized by the presence of gastric mucosa other than the stomach. It can be found at any level of the gastrointestinal (GI) tract, including the biliary tree [1, 2]. GHT in the lower GI tract is uncommon; furthermore, GHT in the proximal large intestine is rare [3]. Diverticular bleeding generally occurs in middle-aged or elderly patients, and in patients treated with anticoagulants or antiplatelet agents [4, 5]. If diverticular bleeding occurs in relatively young patients with no risk factors, the possibility of other diseases should be considered. Here, we report the case of a 17-year-old adolescent boy who was presented with cecal diverticulum perforation and bleeding caused by GHT.
A 17-year-old male visited the emergency room with abdominal pain and hematochezia after undergoing colonoscopy at another hospital. He underwent a small bowel resection and anastomosis due to peritonitis of an unknown cause at the age of 2 years old. During his first hospital consultation, the colonoscope was inserted up to the hepatic flexure, which revealed the presence of fresh blood in the entire colon. In the emergency room, his vital signs showed normal blood pressure with sinus tachycardia (heart rate, 133 beats/min), and his hemoglobin level was 13.6 g/dL. We performed an emergency colonoscopy and found cecal diverticular bleeding. It was successfully controlled using endoscopic clipping (Fig. 1). The patient was discharged 3 days later, without any adverse events.
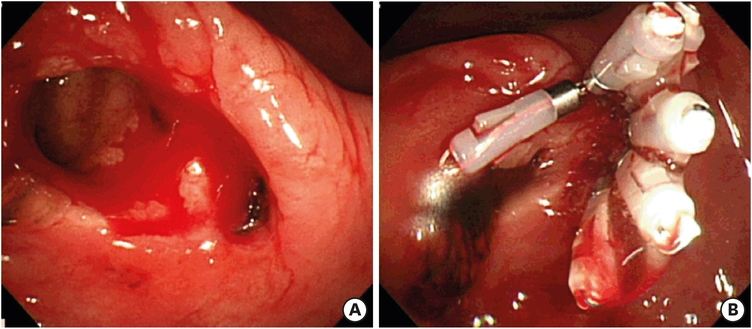
Fig. 1
Colonoscopy bleeding control at first visit. Patient presents with cecal diverticular bleeding (A) and hemostasis has been controlled using hemoclip (B).
Six months later, he visited the outpatient clinic and complained of sustained right lower abdominal discomfort. He had experienced considerable hematochezia one month before visiting the outpatient clinic, but it had subsided without any symptoms, other than the right lower abdominal discomfort. As a result of the hematochezia and sustained right lower abdominal discomfort, we recommended surgery. A colon study showed a diverticulum and external compression in the cecum without any polypoid mass and diverticulum in the colon (Fig. 2).
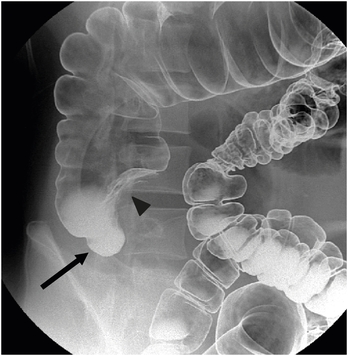
Fig. 2
Colon study finding. There is a diverticulum (arrow) and an external compression (arrowhead) in the cecum. There is no other diverticulum noted in the colon.
Six weeks later, the patient returned with severe and aggravated right lower abdominal pain. His vital signs were stable. Upon examination, the patient had tenderness in the right lower quadrant without signs of peritoneal irritation. His laboratory data were normal except for anemia (hemoglobin level, 7.2 g/dL). Abdominopelvic computed tomography revealed thickening of the ascending and transverse colon, suggesting non-specific colitis, and the presence of multiple lymph nodes that measured less than 1 cm in size in the ileocolic chain, suggesting reactive lymph nodes.
Based on the aggravated symptoms, we decided to perform the surgery. Single-incision laparoscopic ileocecal resection was performed. A cecal perforation was identified. In addition, a moderate adhesion due to his previous operation was also found 20 cm above the ileocecal valve. The entire cecum was resected, and an anastomosis was performed between the ascending colon and terminal ileum. Pathologic findings showed congenital diverticulum with GHT in the cecum and an ulcer with perforation in the cecal area (Fig. 3). Nine days after the operation, the patient was discharged without any complications.
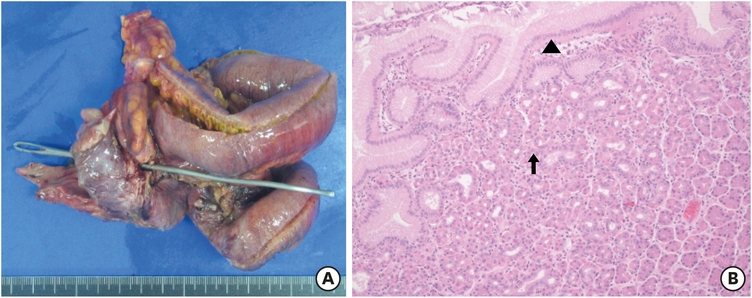
Fig. 3
Gross and microscopic finding. (A) Specimen from the ileocecal resection showing cecal perforation. (B) Pathologic finding showing foveolar-type surface epithelium (arrowhead) with underlying glands, composed of parietal and chief cells (arrow) (haemotoxylin and eosin stain, ×100).
GHT can occur in any part of the body and has been reported to occur anywhere from the esophagus to the anus [6, 7, 8, 9]. There are several hypotheses regarding the pathogenesis of GHT. The congenital theory has been proposed to explain GHT. This theory assumes the failure of the developmental descent of the gastric mucosa during embryogenesis. In contrast, stem cell theory has been proposed for GHT distal to the foregut. This theory assumes the abnormal differentiation of pluripotent stem cells in the GI tract [10]. However, the exact etiology of GHT remains unknown.
The rectum is the most common location in the large intestine for GHT [3]. It rarely occurs in the other parts of the large intestine. When GHT occurs in the large intestine, the most common symptom is hematochezia, which is sometimes accompanied by abdominal pain, diarrhea or both [6].
The symptoms of GHT can be controlled with medications such as H2 antagonists [6]. However, according to previous reports, GHT appears to have the potential to become malignant [3, 11]. Moreover, the risk of malignant transformation may be underestimated. More definitively, surgical or endoscopic removal is the main treatment option, especially for GHT in the lower GI tract. There have been no reports of recurrence after resection of GHT [3].
In this patient with a chief complaint of hematochezia, colonoscopy was performed at the first visit to arrive at a diagnosis, which was eventually determined to be bleeding from the cecal diverticulum. During that time, we could not observe the lesion closely because of active bleeding and clipping. Initially, we did not consider additional examinations because we believed that the possibility of other diseases was low, considering the patient's young age.
However, there are various diseases that can cause rectal bleeding in adolescents, including anal fissures, Henoch-Schonlein purpura, Meckel's diverticulum, infectious colitis, juvenile polyps, inflammatory bowel disease, solitary rectal ulcer syndrome, hemorrhoids, and vascular malformations [12]. The diverticulum itself is rare in adolescence [13]. In addition, diverticular bleeding in adolescence is mostly from Meckel's diverticulum, not from the colon diverticulum. Therefore, in this case, we should have considered additional or repeated examinations and tests such as Meckel scan. However, we did not do so until rectal bleeding recurred and severe abdominal pain was experienced.
We report a case of rectal bleeding caused by GHT in a cecal diverticulum; if the patient's age or symptoms are atypical, then it is crucial to further observe and examine the patient, considering that it may be a rare disease like this case.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.J.Y., S.H.I.
Data curation: K.J.Y., S.H.I.
Investigation: K.J.Y., S.H.I.
Methodology: K.J.Y., S.H.I.
Project administration: K.J.Y.
Resources: K.J.Y.
Supervision: K.J.Y.
Writing - original draft: K.J.Y., S.H.I.
Writing - review & editing: K.J.Y., S.H.I.
