

Purpose
Ovarian mucinous cystadenocarcinoma is rare in adolescent population and reports are scarce in Korea. The aim of this study was to identify the clinicopathologic features and prognosis of adolescent ovarian mucinous cystadenocarcinoma.
Methods
Adolescent patients who were diagnosed with ovarian mucinous cystadenocarcinoma between 2001 and 2012 in Seoul National University Children Hospital were included. We retrospectively reviewed medical records of demographics, preoperative evaluation, tumor characteristics, and prognosis of patients.
Results
Among 5 patients, none of them reported family history of cancer or underlying disease relevant to malignancy. The median follow-up period was 13.3 years. The mean age at the time of diagnosis was 15.4 years. The mean size of the tumor was 26 cm. Only one patient had neoadjuvant chemotherapy. All patients underwent surgical treatment. One patient underwent total abdominal hysterectomy and bilateral salpingo-oophorectomy for cytoreductive surgery and 4 patients underwent fertility sparing surgery. Three patients had platinum-based adjuvant chemotherapy. One patient suffered recurrence and eventual death and 4 patients are in disease free survival status.
Conclusion
Although ovarian mucinous cystadenocarcinoma in adolescent is rare, we should suspect the presence of it in case of adolescent intraabdominal large mass. As adolescent patients undergo fertility preserving surgery, serial and careful follow-up is necessary.
Ovarian mucinous cystadenocarcinoma is rare in adolescent population and reports are scarce in Korea. The aim of this study was to identify the clinicopathologic features and prognosis of adolescent ovarian mucinous cystadenocarcinoma.
Adolescent patients who were diagnosed with ovarian mucinous cystadenocarcinoma between 2001 and 2012 in Seoul National University Children Hospital were included. We retrospectively reviewed medical records of demographics, preoperative evaluation, tumor characteristics, and prognosis of patients.
Among 5 patients, none of them reported family history of cancer or underlying disease relevant to malignancy. The median follow-up period was 13.3 years. The mean age at the time of diagnosis was 15.4 years. The mean size of the tumor was 26 cm. Only one patient had neoadjuvant chemotherapy. All patients underwent surgical treatment. One patient underwent total abdominal hysterectomy and bilateral salpingo-oophorectomy for cytoreductive surgery and 4 patients underwent fertility sparing surgery. Three patients had platinum-based adjuvant chemotherapy. One patient suffered recurrence and eventual death and 4 patients are in disease free survival status.
Although ovarian mucinous cystadenocarcinoma in adolescent is rare, we should suspect the presence of it in case of adolescent intraabdominal large mass. As adolescent patients undergo fertility preserving surgery, serial and careful follow-up is necessary.
Ovarian neoplasms in the pediatric patients are rare and the incidence is 2.6 per 100,000 per year [1]. Ovarian neoplasms include germ cell tumors, surface epithelial tumors, and sex cord-stromal tumors. Most of the ovarian tumors in pediatric population is germ cell tumors, with the frequency of 58%–70%. The frequency of surface epithelial tumor is 15%–19% and that of sex cord-stromal tumor is 9%–18%. The frequency of miscellaneous tumor is 5%–9% [2]. In adult, the most common ovarian neoplasm is surface epithelial tumor, which accounts for 80%–90%. There is difference in frequency of ovarian neoplasm between adolescent and adult population. Few reports reported regarding surface epithelial neoplasms in adolescent patients, especially in Korean. This study aimed to analyze the clinicopathologic features through cases series of adolescent ovarian mucinous cystadenocarcinoma in a single center.
This study involved adolescent patients diagnosed with ovarian mucinous cystadenocarcinoma in Seoul National University Children Hospital between 2001 and 2012. We included patients aged less than 18 years-old at diagnosis. We retrospectively reviewed patient's data from electronic medical records on sex, age at diagnosis, symptom duration, and family history of cancer, underlying disease, tumor location, tumor size, tumor marker, pathologic results, chemotherapy, last follow-up date, date of death, 5-year survival, recurrence, and mortality. Symptom duration was defined as the period from initial symptom onset to diagnosis. Tumor size was defined as the longest diameter from the gross pathologic report. Pathologic stages were converted to American Joint Committee on Cancer (AJCC) 8th edition stages based on tumor invasion depth and the number of lymph nodes showing metastasis. AJCC is an organization known for defining cancer staging standards [3]. Patients who received neoadjuvant and adjuvant chemotherapy were included. The last follow-up was defined as the last outpatient visit. Treatment was performed according to the international guidelines of ovarian cancer. This study was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB number: 1811-053-983).
The number of included patients was 5. The mean age of patients was 15.4 years (Table 1). Main symptom and sign of patients was abdominal distension. Duration of symptom was between 1 and 4 months. None of the patients had family history of cancers. Preoperative tumor markers including serum cancer antigen 125 (CA-125) and carcinoembryonic antigen was evaluated. Three out of five patients were measured in normal range of CA-125 level (5–45 U/mL). The preoperative values of CA-125 and serial follow-up values of each patient were collected and depicted in graph (Fig. 1). In all patients, CA-125 level decreased after operation. In patients #5, CA-125 level decreased after operation, however it increased slowly even after adjuvant chemotherapy. At the time of tumor recurrence, CA-125 level peaked again, measured 173.4 U/mL. Ultrasonography (USG) and computed tomography (CT) were performed in all patients and magnetic resonance imaging (MRI) was performed in 2 patients. Three patients had ovarian cancer in left and 2 patients had in right. Average 28 cm sized multiseptated cystic mass was observed and some contained solid portion in mass. Patient #3 showed nodular infiltration of mesentery which implies the possibility of peritoneal seeding. Patient #5 displayed lymph node enlargement in para-aortic area and renal hilum. In most of the cases, we suspected malignant ovarian epithelial tumor according to imaging.
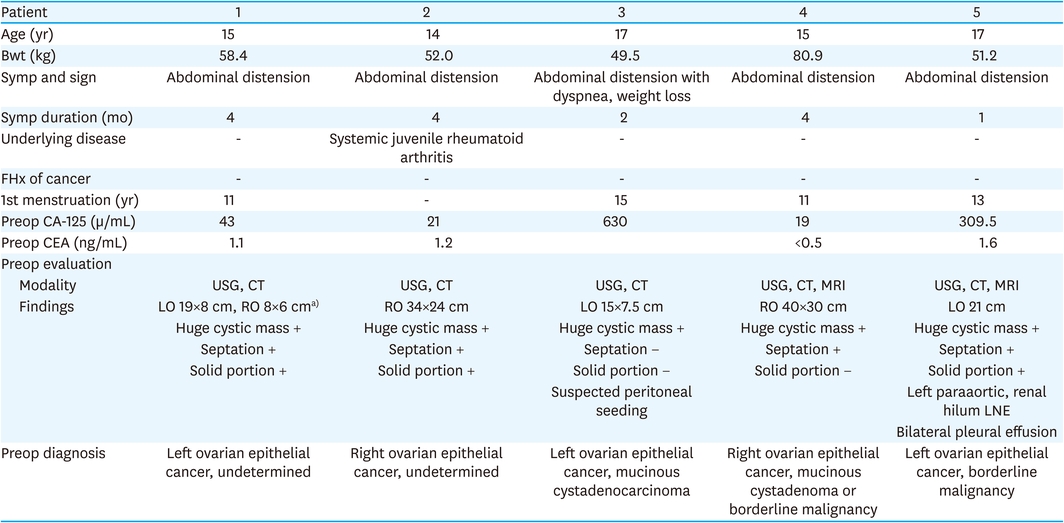
Table 1
Demographics and preoperative evaluation
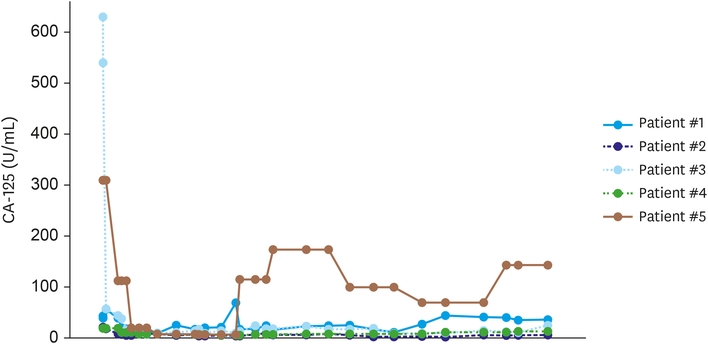
Fig. 1
Interval change of CA-125 level of patients.
CA-125, cancer antigen 125.
Patients with ovarian mucinous cystadenocarcinoma undergo neoadjuvant chemotherapy, cytoreductive surgery, and adjuvant chemotherapy according to the severity of the disease (Table 2). Patient #3 with suspected peritoneal seeding underwent neoadjuvant treatment, which was 2 cycles of etoposide, ifosfamide, cisplatin. However, the response of the treatment was progressive disease state according to the response evaluation criteria in solid tumors criteria. All patients underwent washing cytology and there were no malignant cells in cytologic findings. Patient #1 underwent left ovarian cystectomy for carcinoma in order to preserve fertility and right ovarian cystectomy to remove the synchronous right benign tumor. Patient #2 had right oophorectomy. In order to preserve fertility, unilateral oophorectomy was done. Patient #3 underwent total abdominal hysterectomy (TAH), bilateral salpingo-oophorectomy (BSO), and pelvic lymph node dissection (PLND). Left ovarian tumor was implanted to uterus and large amount of ascites was observed. In addition, she underwent intraperitoneal high-dose cisplatinum chemotherapy. Among dissected 14 nodes during surgery, no node had involvement of tumor cell. Patient #4 had right salpingo-oophorectomy surgery. Patient #5 underwent left salpingo-oophorectomy (LSO), PLND, and paraaortic lymph node dissection (PALND) by laparoscopic approach. As some lymph node enlargements were observed in the preoperative CT and MRI, lymph node dissection and biopsy were performed. There was no evidence of malignant cell in dissected lymph nodes. During the surgery, ovarian cyst ruptured and cystic fluid spilled out during the aspiration. The staging of epithelial ovarian cancer was done by standardized and contemporary cancer staging system, which is AJCC 8th staging system. Final pathology was mucinous type cystadenocarcinoma in all patients. Patient #1 had synchronous contralateral ovarian mucinous type cystadenoma. Two patients were in stage Ia and 2 patients were in stage Ic. One patient was in stage IIa. Adjuvant chemotherapy was performed except for 2 patients with stage Ia.
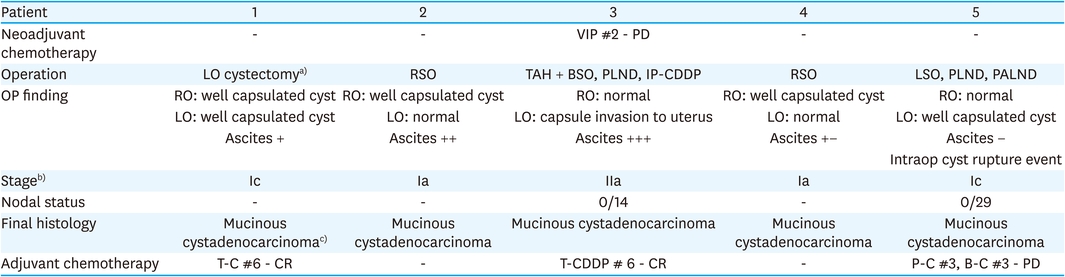
Table 2
Treatment, staging and pathology
The median follow-up period was 13.3 years (Table 3). We found peritoneal seeding with multiple lymph node enlargement in patient #5 in postoperative 6 months. Because cancer progressed during the time of adjuvant chemotherapy, adjuvant chemotherapy by alternating regimen was planned. However, the patient discharged voluntarily. Eventually patient died in postoperative 15 months. Patient #2 underwent further 3 times of operations. Biopsy of liver, spleen, paraaortic lymph node was done in postoperative 1 month. There was no tumor involvement in pathology. Tumorectomy of liver was done twice in postoperative 45 months and 73 months, which all resulted inflammatory myofibroblastic tumor. There was no evidence of recurrence of ovarian mucinous cystadenocarcinoma.
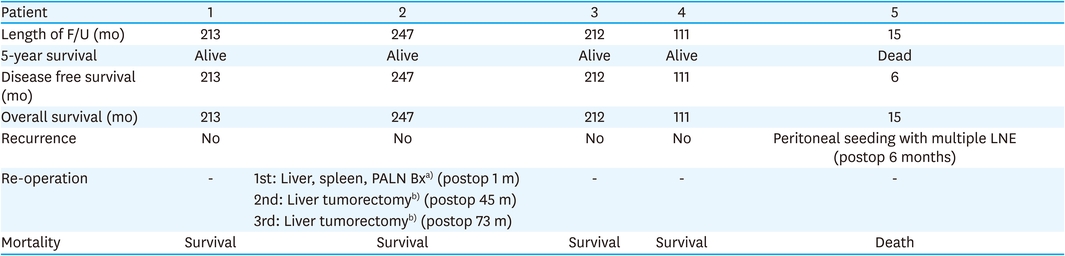
Table 3
Prognosis
The patient #5 is demonstrated as a representative case. A previously healthy 17-year-old female patient suffered from abdominal distension. She was diagnosed with left ovarian epithelial cancer. According to the CT image, 21 cm sized huge cystic mass with septation and solid portion inside was observed (Fig. 2A). Also, left paraaortic and left renal-hilum lymph node enlargement were identified (Fig. 2B). She underwent LSO, PLND, and PALND. The pathology of left ovary was mucinous cystadenocarcinoma. In microscopic view, multilocular cystic spaces lined by intestinal type mucinous epithelium with occasional papillary projection. Some foci of destructive stromal invasion are occasionally seen, so the pathologic diagnosis is mucinous cystadenocarcinoma (Fig. 3).
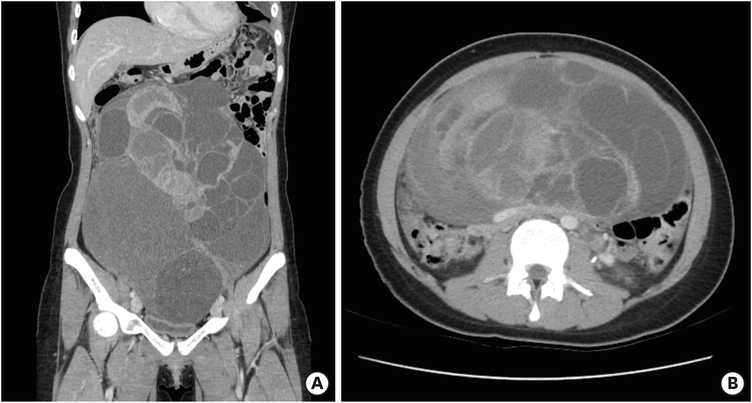
Fig. 2
Computed tomography of patient #5. (A) Coronal image, 21 cm-sized huge cystic mass with septation and solid portion, (B) axial image, left paraaortic and left renal-hilum lymph node enlargement.
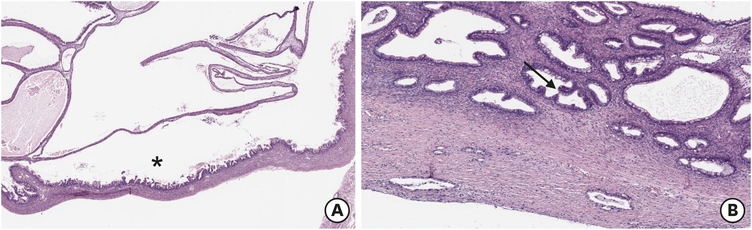
Fig. 3
Microscopic view of ovarian mucinous cystadenocarcinoma (hematoxylin and eosin microscopy) in patient #5. (A) Multilocular cystic spaces are lined by intestinal type mucinous epithelium with occasional papillary projection(*). (B) Some foci of destructive stromal invasion are occasionally seen (arrow). So, the pathologic diagnosis of this case is mucinous carcinoma.
This case series delt with 5 patients with epithelial ovarian cancer. The mean age at diagnosis was 15.4 years. Most of the patients complained abdominal distension as a symptom. According to the other reports, abdominal pain is the most common presenting symptom, followed by a palpable abdominal or pelvic mass [4]. Some patients also present with nausea, vomiting, poor appetite, weight loss, and urinary frequency. Tenderness is likely the symptom of torsion, hemorrhage, or rupture of ovarian tumors [5]. Endocrine abnormality such as menstrual irregularity is another manifestation of hormone producing ovarian tumors [6]. Children with a palpable mass or precocious puberty are related to high probability of malignancy [7]. Ovarian torsions are likely to have no pathologic lesion or have benign cyst. Acute onset of pain or tenderness is sign of benign ovarian tumors rather than malignant tumors [8]. However, clinical symptoms and signs are nonspecific and not a factor for differential diagnosis of ovarian tumor.
Imaging features at USG, CT, MRI are helpful for identification of types of tumors and malignancy potential. Epithelial tumors are rare before menarche since hormonal stimulation cause development of tumors [9]. Papillary projections are more common in borderline epithelial tumors than in benign cystadenoma and malignant epithelial tumors. Malignant epithelial tumors are usually large mass with thick and irregular wall or septa and solid portion with necrosis. In this paper, masses were evaluated in preoperative stage using sonography, CT, and MRI. Patient #3 had no septation and solid portion in mass, however, peritoneal seeding was suspected in the CT scan.
There is no conclusive standard size for suspect malignancy. According to some studies, the relationship of the size of the masses and ovarian malignancy was not confirmed. This is because the size of the mass includes cystic portion of the mass, however, the solid portion of the mass is relevant to the malignancy [10]. Mucinous type usually includes large, multilocular cystic mass with variable attenuation at CT and variable signal intensity at MRI [11].
According to the American Society of Clinical Oncology guideline, surgical cytoreduction to R0 is the mainstream of the treatment, followed by adjuvant chemotherapy. R0 resection removes all macroscopic disease [12]. For primary cytoreductive surgery, surgeon conducts peritoneal washing, TAH, BSO or USO, and debulking surgery, which includes lymph node dissection, omental biopsy, and appendectomy. Neoadjuvant chemotherapy is considered when optimal cytoreduction is unlikely or when accompanying high perioperative morbidity and mortality. The adjuvant therapy for ovarian cancer is not recommended in stage IA or IB because 5-year survival rates are greater than 90% after surgical treatment [13, 14]. Patients with advanced stage are recommended to have adjuvant therapy which is carboplatin/taxane for 3 to 6 cycles. Among 5 patients, one patient who were suspected of peritoneal seeding had neoadjuvant chemotherapy. Because neoadjuvant chemotherapy was not effective, only 2 cycles were conducted. TAH, BSO and PLND was performed for cytoreductive surgery. Except for 2 patients who were diagnosed as stage Ia, 3 patients had adjuvant chemotherapy.
Fertility sparing procedures is considered appropriate for maintaining fertility in young patients especially adolescents. According to the International Federation of Gynecology and Obstetrics and the American College of Obstetricians and Gynecologists, unilateral salpingo-oophorectomy or ovarian cystectomy is suggested who desire fertility. This guideline is applicable in that there is more risk than benefit of resecting clinically normal lymph nodes, random peritoneal biopsies, or removing clinically uninvolved tissue such as uterus and ovary in stage [15, 16]. However, the rate of recurrence after fertility sparing procedures varies from 0% to 37.5% according to the researches. The rate of recurrence was even higher after an ovarian cystectomy, which varies from 12.0% to 37.5% [17, 18, 19, 20, 21]. This implies that patients who underwent fertility sparing procedure need close follow-up. In our study, 3 patients underwent unilateral salpingo-oophorectomy and one patient underwent bilateral ovarian cystectomy. Serial follow-up with imaging modality and tumor marker was done. For 3 patients, there was no recurrence after more than 15 years of follow-up. One patient suffered recurrence at postoperative 6 months and peritoneal seeding with multiple lymph node enlargement was observed. Adjuvant chemotherapy was not effective and patient died at postoperative 15 months.
Assay of serum tumor markers is method for the differential diagnosis. The serum AFP level is elevated in patients with germ cell tumor [22]. The β-hCG is associated with choriocarcinoma and embryonal carcinoma. The LDH level is related to dysgerminoma and CA-125 is related to epithelial tumors. Elevation of tumor markers is associated with ovarian malignancy; however, negative tumor marker does not exclude the possibility of malignancy [9, 23, 24]. CA-125 is recommended in surveillance and follow-up of ovarian epithelial tumor. The sensitivity and specificity of CA-125 for detecting recurrences range from 62% to 94% and from 91% to 100%, respectively [21]. CA-125 is a protein associated with epithelial ovarian malignancies, often expressed at lower levels in benign tumors. Elevation of CA-125 level can also be observed in adolescent patients with benign gynecologic conditions including noncommunicating uterine horns, endometriosis, pregnancy, and pelvic inflammatory disease, thus confusing the picture in this patient population. Therefore, as opposed to the 35 U/mL threshold in postmenopausal women, the American Congress of Obstetricians and Gynecologists has used a CA-125 threshold of greater than 200 U/mL on the basis of expert opinion for referral of premenopausal women to gynecologic oncologists for evaluation of malignancy; however, no evidence-based threshold is currently available. Gynecology providers should integrate the CA-125 level and other clinical factors in determining risk for malignancy [25]. In this report, preoperative evaluation and follow-up of CA-125 was done. In preoperative evaluation, 2 patients showed elevation of CA-125 level. In patient 5, when the recurrence was suspected at CT scan, CA-125 level elevated upto 173.4 U/mL. Therefore, this marker is imperative for surveillance.
Although ovarian mucinous cystadenocarcinoma in adolescents is rare, we should suspect the presence of it in case of adolescent intraabdominal large mass. As adolescent patients undergo fertility preserving surgery, serial and careful follow-up is necessary.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.H.Y.
Data curation: Y.H.B.
Formal analysis: C.A.
Investigation: C.A.
Methodology: K.H.Y.
Project administration: K.H.Y.
Resources: Y.H.B.
Software: C.A.
Supervision: K.H.Y.
Validation: Y.H.B.
Visualization: C.A.
Writing - original draft: C.A.
Writing - review & editing: Y.H.B.
