Department of Surgery, Chungnam National University School of Medicine, Daejeon, Korea.
Copyright © 2013 Korean Association of Pediatric Surgeons
*Voluntary bowel movement: feeling of urge, capacity to verbalize, hold the bowel movement
†Soiling: Grade 1 occasionally (once or twice per week); Grade 2 every day, no social problem; Grade 3 constant, social problem
+Constipation: Grade 1 manageable with diet; Grade 2 requires laxatives; Grade 3 resistant to diet and laxatives

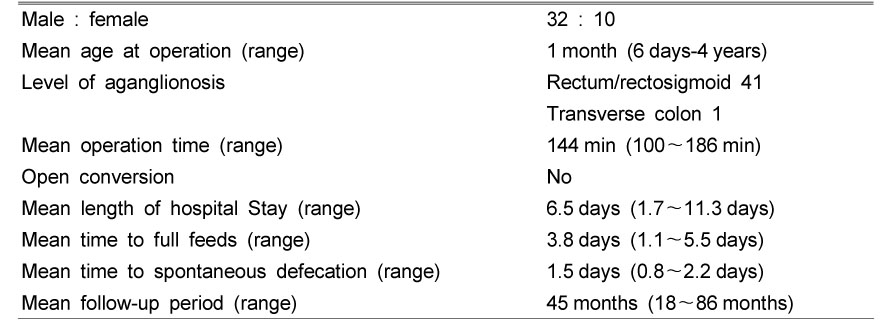
General Patients and Surgical Characteristics
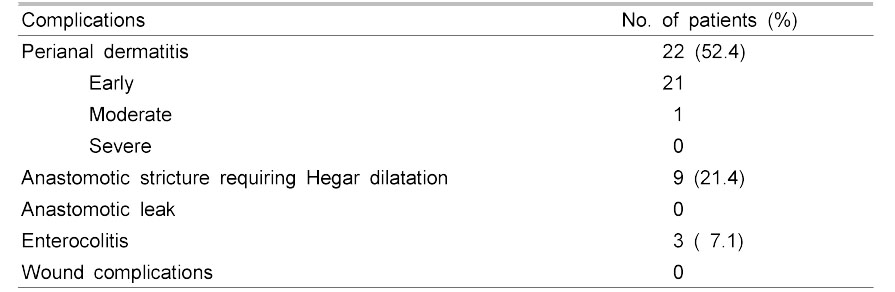
Early Postoperative Complications (<3 Months after Surgery)
Late Postoperative Complications and Long-term Outcomes (>3 Months after Surgery)
Functional Results of Krickenbeck Assessment (N=32 Patients >3 Years Old)
*Voluntary bowel movement: feeling of urge, capacity to verbalize, hold the bowel movement
†Soiling: Grade 1 occasionally (once or twice per week); Grade 2 every day, no social problem; Grade 3 constant, social problem
+Constipation: Grade 1 manageable with diet; Grade 2 requires laxatives; Grade 3 resistant to diet and laxatives
*Voluntary bowel movement: feeling of urge, capacity to verbalize, hold the bowel movement
†Soiling: Grade 1 occasionally (once or twice per week); Grade 2 every day, no social problem; Grade 3 constant, social problem
+Constipation: Grade 1 manageable with diet; Grade 2 requires laxatives; Grade 3 resistant to diet and laxatives