
The risk of acute abdomen in neonates and infants is generally increased due to advanced maternal age and neonatal intensive care unit care development. Enterostomy is a safe procedure for acute abdomen in neonates and infants. However, there is no consensus for the optimal timing of enterostomy closure (EC). A few considerations should be reviewed for deciding the timing of stoma closure to obtain the best outcome. Distal loopography is commonly performed upon examination to ascertain the existence of a distal passage after EC, detect signs of disease-specific complications, and assess the need of surgery in addition to EC. Pathology review is also one important pre-closure consideration. When the incidence of a hypoganglionosis or an aganglionosis combined with acute abdomen is observed in neonates and infants, thorough examinations should be performed to conclusively determine whether there is no passage disturbance of the distal bowel. Refeeding not only provides information about chance to grow, electrolyte imbalance correction, and proximal and distal bowel size match, but also provides information about distal bowel passage when there is a doubtful distal loopography or pathology result. Early closure enables growth spurt with the correction of water/electrolyte imbalance. It potentially reduced medical costs, less discrepancy between proximal and distal bowel size. Some factors favoring a late stoma closure may be due to less postoperative complications, early recovery, shorter time of total parenteral nutrition after EC, and decreased length of hospitalization after the EC. Some studies have shown controversial results. In summary, a pre-closure evaluation is imperative to assure the safety of an EC. The optimal timing of an EC remains controversial. For this reason, individualized approach is needed after reviewing the general condition of each patient. Further prospective study on optimal timing of stoma closure including a randomized clinical trial is needed.
Citations
Inguinal hernia in early infant is a challenging surgical condition. This study aims to evaluate the efficacy and safety of laparoscopic inguinal hernia repair (LH) for small babies in corrected age 3 months compared with the traditional open inguinal hernia repair (OH).
Medical records were retrospectively reviewed in 232 pediatric patients under corrected age 3 months who underwent inguinal hernia repair from January 1, 2013 to December 31, 2015. The chi-squared and Fisher's exact test were used to analyze the results of the study.
As for operative time, in unilateral/bilateral inguinal hernia repair, OH is faster than LH (p<0.05 vs. p=0.06). But operation time gap is shorter in bilateral hernia than unilateral hernia. As for operation site, bilateral inguinal hernia case was more performed in LH than OH (p<0.05). For comparison with the spontaneous breathing recovery time, there was no statistical difference between the two techniques (p=0.96). As for the recurrence rate, no significant difference was observed between the two techniques (p=0.36), whereas the relative risk of recurrence was higher for OH compared with LH (OR=1.56).
LH is also feasible and safe procedure as OH for small babies in corrected age 3 months for experienced pediatric surgeons.
Citations
The single stage transanal pull-through (SSPT) for Hirschsprung’s disease is becoming the most popular procedure. This single center study compared the result of single stage operation with two-stage operation for Hirschsprung’s disease in neonates.
We retrospectively reviewed medical records of all patients who were diagnosed as Hirschsprung’s disease and underwent SSPT or two-stage operation operation in Asan Medical Center between January 2003 and July 2014.
There were 17 SSPT and 28 two-stage operation. The mean age of SSPT group was 14.2±7.1 days, and the mean age of two-stage operation group was 15.4±8.6 days for stomy formation, and 188.6±36.3 days for Duhamel operation. The operation time of SSPT was shorter than Duhamel operation (145.0±37.0 minutes vs. 193.0±36.0 minutes, p<0.001). The mean follow-up period of SSPT and two-stage operation was 35.5±34.9 months (range, 2-132 months) and 56.6±35.5 months (range, 1-121 months), respectively. Defecation problem rate such as fecal soiling or fecal impaction showed no significant difference between the two groups (p=0.719). Two SSPT patients required botulinum toxin injection due to rectal stenosis. Three patients of SSPT group underwent re-do endorectal pull-through due to remnant aganglionic or hypoganglionic bowel.
The SSPT showed shorter hospital days. However, few patients experienced rectal stenosis, but were manageable with botulinum toxin injection. The SSPT requires experienced-pathologist, as well as surgeon, because intra-operation pathology reading is critical for appropriate SSPT. SSPT is a feasible and reasonable option to treat Hirschsprung’s disease.
Citations
This is a survey on congenital posterolateral diaphragmatic hernia, conducted by Korean Association of Pediatric Surgeons (KAPS). A registration form for each patient during the 5-year period between 2010 and 2014 and a questionnaire were sent to each member. Twenty-six members in 16 institutions returned completed forms. Total patients were 219. Prenatal diagnoses were done in 181 cases (82.6%). Preoperative mortality was 11.4%. Minimal invasive surgery was done in 61 cases (31.8%). Risk factors related with death were Apgar score, oxygenation index, preoperative pH and bicarbonate, O2 saturation, the presence of hernia sac, and the size of defect. The neonatal survival and 1-year survival of total patients were 77.6% and 75.3%.
Citations
Infantile hypertrophic pyloric stenosis (IHPS) is one of the common surgical abdomen in infancy, characterized by progressive non-bilious vomiting. The etiology is unknown, but it likely develops after birth. The pylorus of the stomach becomes thick and triggers progressive vomiting. Abdominal ultrasonography (US) is widely used as a diagnostic tool. Currently, there is a rare IHPS patient with severe metabolic derangement because of general use of abdominal US and its accuracy. We experienced a natural course of a 62- day-old male infant with IHPS who was suffering from intermittent vomiting, loss of weight but had not been properly treated for 1 month. It is needed to make an effort to diagnose differentially in recurrent vomiting infant and check-up regularly, and also educate parents properly.
Citations
Gastric teratoma is an extremely rare tumor that accounts for less than 1% of all teratomas. Gastric teratoma is mostly presented as a palpable abdominal mass, and is rarely accompanied with gastrointestinal bleeding such as melena or hematemesis. A 5-month-old male infant was brought with a history of pale facial color and dark-colored stool. The hemoglobin level was at 6.1 g/dL, with melena having begun 1 month previous. Upper gastrointestinal endoscopy revealed a polypoid mass with bleeding at the upper body and lesser curvature of the stomach. Wedge resection of the stomach was performed and histopathological analysis confirmed the mass to be a mature cystic teratoma. There was no recurrence after the operation during follow-up.
Citations
The perforation and subsequent panperitonitis as one of the complications of a Meckel diverticulum is a rare complication, especially in infants. Complication of Meckel diverticulum, preoperative and operative patient's mean age is about 5 years old. A 13-month-old male infant presented at our emergency room with currant jelly stool of about 24 hours duration. Intussusception or bacterial enteritis was initially suspected. Gastrointestinal ultrasonography showed no evidence of intussusception or appendicitis. On the 3rd hospital day, he suddenly showed high fever and irritability. Abdominal CT suggested intraperitoneal and retroperitoneal abscess with air collection due to possible bowel perforation. The final diagnosis of perforation of Meckel diverticulum was made by laparoscopy and biopsy. We report a very rare case with perforation of Meckel diverticulum in infant period.
Citations
Long time total parenteral nutrition (TPN) can induce irreversible liver damage. In this study, we investigated the associated factors of parenteral nutrition associated cholestasis (PNAC) in neonates.
We retrospectively reviewed 227 neonates (male:female=110:117) those who had received TPN over 2 weeks from March 2010 to February 2014. PNAC was defined as direct bilirubin was higher than 2.0 mg/dL without any cause except TPN.
Overall incidence was 28.6%. PNAC was frequently developed in younger gestational age with lower birth weight. Episodes of sepsis, underlying bronchopulmonary dysplasia, history of necrotizing enterocolitis, and experience of gastrointestinal surgery increase the incidence of PNAC. PNAC was directly associated the duration of TPN and long period to full enteral feeding, reaching 60 and 150 mL/kg/day. Overall mortality rate was 9.7%. It was higher in PNAC group despite PNAC was not the primary cause of death. All survivors were recovered from cholestasis with encourage of enteral nutrition.
PNAC in neonate was associated with younger gestational ages and lower birth weights, duration of TPN, or who experienced sepsis, necrotizing enterocolitis, gastrointestinal surgery or bronchopulmonary dysplasia.
Hypertrophic pyloric stenosis (HPS) is the most common infantile surgical condition and the standard treatment is open pyloromyotomy. Recently, laparoscopic techniques have rapidly advanced, and the laparoscopic approach has become widely adopted by pediatric surgeons. The aim of this study was to compare the clinical outcomes between open and laparoscopic pyloromyotomy. We retrospectively evaluated outcomes of pyloromyotomy for HPS by the open (OP) and the laparoscopic (LP) method. The procedures were performed at the Samsung Medical Center between September 2001 and March 2009. We analyzed patient age, sex, birth weight, length of hospital stay, postoperative length of stay (LOS), operating time, time to feeding commencement, postoperative vomiting frequency, the time to full feeding without vomiting, and surgical complications. A total of 54 patients were included in the study. There were 26 OP and 28 LP patients. There was no statistically significant difference in age, sex, birth weight, operating time, postoperative emesis. In contrast, postoperative LOS in the LP group was statistically significantly shorter than that in the OP group (2.0 vs. 3.3 days,
Citations
The clinical characteristics of fistula-in-ano in infants are different from those of older children, and its treatment remains controversial. We suggest that fistula-in-ano in infants has a congenital etiology. To verify this hypothesis and to settle the controversies regarding fistula-in ano in infants, a retrospective analysis of 29 patients less than 2 years of age with anal fistulae treated between 1994 and 2009 at Samsung Changwon Hospital were reviewed retrospectively. Twenty two patients were male and mean age at diagnosis was 7.2±5.2 months. Eleven out of 22 cases had previous surgical drainage for perianal abscess. 18 patients had fistulotomy (81.8%) and four had fistulectomy (18.2%). Cryptotomies with fistulectomy were performed in 10 patients (45.5%) who had involved crypt. There was one recurrence. These results suggest that fistula-in-ano in young children less than two years of age is different from those in older children or adults. Fistulotomy is suggested to be the recommended treatment of choice. A future study involving non-operative management would be required to explore all treatment options.
Citations
Extraosseous Ewing's sarcoma is a rare primary malignant soft tissue tumor which is histologically identical to Ewing's sarcoma. This tumor tends to involve the soft tissue of the lower extremity and paravertebral region of adolescents and young adults but particularly rare in infants. We recently experienced a case of extraosseous Ewing's sarcoma which presented in the left arm of 4 months infant.
Accessory cervical thymic tissue has been rarely reported. However, it should be included in the differential diagnosis of neck masses in children, along with branchial anomalies, lymph nodes and other tumors. This lesion occurs along the descending line of the thymus between the angle of mandible and superior mediastinum. A 2-month-old infant presented with an asymptomatic left sided neck mass. MRI revealed a well defined homogeneous mass in the deep lobe of left parotid gland. At operation, an easily identified soft tissue mass was found in the left submandibular area, measuring 3 × 1.5 cm. It was completely excised. Microscopic examination revealed normal thymic tissue.
Recently, the survival rates of extremely low-birth-weight (ELBW) infants have improved with the development of neonatal intensive care. However, these infants were susceptible to intestinal perforation due to prematurity, fluid restriction, and injection of indomethacin, etc. Because of the risks of transportation, anesthesia and surgery itself, peritoneal drainage has been compared with laparotomy. Through our experience, we investigate the usefulness of peritoneal drainage retrospectively. From 1997 to 2007, six ELBW (M:F=5:1) underwent primary peritoneal drainage for intestinal perforation. Their median birth weight was 685 g (405~870) and gestational age was 25+1 weeks (24+3~27+0). We noticed the intestinal perforation at median 10.5 days (8~18) after birth, and placed Penrose drain or Jackson-Pratt drain through right lower quadrant incision under local anesthesia. The cause of intestinal perforation was necrotizing enterocolitis in one patient, but that of the others was not clear. Three patients who showed normal platelet count and stable vital signs recovered uneventfully. Two patients (birth weight less than 500 g) who showed unstable vital signs and low platelet count (12,000 / mm3 to 30,000 / mm3) expired despite aggressive resuscitation. One patient required laparotomy due to persistent intestinal obstruction after drain removal and survived. Our experience shows that peritoneal drainage was an acceptable treatment for ELBW infants and the prognosis was related to vital sign and platelet count at the time of intestinal perforation, and birth weight.
Citations
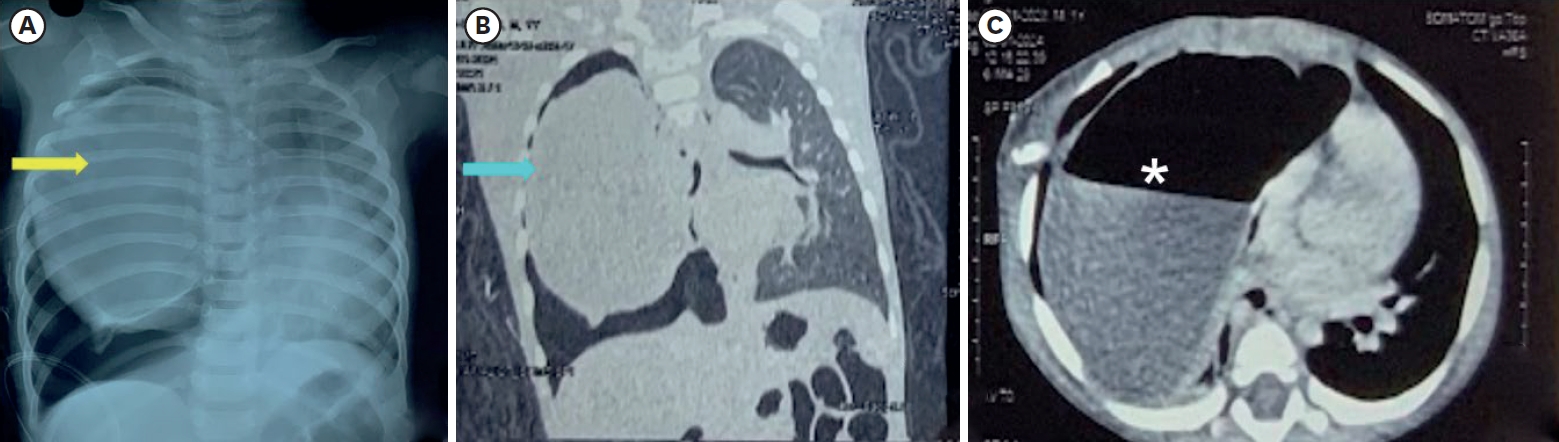
An 1-month old female newborn was admitted to our hospital because of jaundice which occurred at 2 days after birth. Plain chest X-ray and chest CT revealed a collapsed right middle lobe and lobar emphysema was suspected. Right upper lobectomy of the lung was done and pathologic findings showed an infantile lobar emphysema. After the operation, the newborn was discharged without complication and was followed up through the out patient clinic. Infantile lobar emphysema is rare and male dominant. Left upper lobe of the lung is the most prevalent site. Patients with infantile lobar emphysema complain of respiratory symptoms. We report one case of infantile lobar emphysema on right upper lobe of lung, in a female with no respiratory symptoms.
A newborn male baby was transferred to our hospital with a left inguinal mass. The mass was huge measuring 10 x 10 cm, engorged, and dark-blue colored as a result of internal hemorrhage. Unstable vital signs were combined with DIC and acute renal failure. Emergency operation was performed because of the suspicion of bowel perforation. The peritoneal cavity was full of ascitis and the distal jejunum had a 0.5 cm perforation. Segmental resection of the jejunum and incisional biopsy of the inguinal mass were performed. On pelvic and thigh MRI, the mass protruded into pelvic cavity and encircled large vessels and nerves of the thigh. Pathologic diagnosis was congenital infantile fibrosarcoma. Fifteen days after operation, primary tumor excision was undertaken. The second look operation, performed after 6 times VAC chemotherapy, revealed no remained malignant cell on microscopic section. The baby has been followed closely for the last eight months.
Necrotizing enterocolitis (NEC) is usually a disease of premature infants, but occasionally it affects the term neonate. Twenty-five infants with NEC were treated at Asan Medical Center between January 2000 and December 2002. and 13 of them were term infants. In each case, the diagnosis of NEC was established by a clinical illness fulfilling the Bell's stage II or III NEC as modified by Walsh or by surgical findings. There were six males and seven females. The birth weight was from 1,960 to 3,700 g. The age at diagnosis was from 1 to 40 days. Four patients had congenital heart disease; one of them had hypothyroidism and cleft palate. Abdominal distension was present in all, and bloody stools in four. One patient had history of hypoglycemia, three had Rota viral infection. Eight patients had leucopoenia (<5.0 × 109/L), Seven had thrombocytopenia (<100 × 109/L), and three severe thrombocytopenia (<50 × 109/L). Laparotomy was required in 10 of the 13 patients. Indications for operation in acute phase were failure to respond to aggressive medical therapy in five, and perforation in three patients. There were two late phase operation for intestinal stricture and fistula. There was no operative complications. Ten of thirteen patients survived (76.9%). Two patients died of septic complication. There was a delayed death due to heart failure. There was a significant difference in survival according to platelet count (50 × 109/L) (p<0.05). Congenital heart disease and Rota viral infection is associated with NEC in term infants and thrombocytopenia and leucopenia in the course may be surgical indications.
When jaundice persists for more than 14 days postnatally, the early diagnosis of surgical jaundice is important for the prognosis in extrahepatic biliary atresia after draining procedure. The role of diagnostic laparoscopy to differenctiate medical causes of jaundice from biliary atresia is evaluated in this report. Four patients with prolonged jaundice have been included in this study. When the gallbladder was not visualized we proceeded to laparotomy. In patients with enlarged gallbladder visualized at laparoscopy, laparoscopic guided cholangiogram was performed, and laparoscopic liver biopsy was done for those who had a patent biliary tree. Two patients had small atretic gallbladder and underwent a Kasai hepato-portoenterostomy. One patients showed a patent gallbladder and common bile duct with atresia of the common hepatic and intrahepatic ducts, and they underwent a Kasai hepatic-portoenterostomy. One patient showed an enlarged gallbladder and laparoscopic-guided cholangiogram were normal. Laparoscopic liver biopsy was performed. There were no complications. Laparoscopy wth laparoscopic-guided cholangiogram may be a valuable method in accurate and earlier diagnosis in an infant with prolonged jaundice.
The purpose of this study is to evaluate the applicability of intravenous atropine sulfate therapy in infantile hypertrophic pyloric stenosis (IHPS). From 1998 to 2000 among 35 cases of IHPS, pyloromytomy was performed in 13 (Group A), and intravenous atropine was given as a primary therapy in 22 cases (Group B). In group A, all cases were cured completely. In group B, 13 (59 %) out of 22 cases were successfully treated with atropine, but 9 were failed therapy, and required operation. The recovery period to normal feeding and the hospital stay of the successful atropine group were longer than those of pyloromyotomy, 8.6 days vs. 2.9 days and 13.2 days vs. 4.1 days, respectively. In conclusion, intravenous atropine therapy did not replace pyloromyotomy, but it might be an alternative for the selected patients with contraindications for operation.
Infantile hypertrophic pyloric stenosis (IHPS) a common childhood disorders characterized by nonbilious projectile vomiting, an olive shaped mass in the right upper quadrant of the abdomen and visible gastric peristaltic wave in the upper abdomen. Its etiology and pathogenesis are not clear but abnormal nerve distribution of the pylorus has been postulated2-6. We performed immunocytochemical staning to the pyloric muscle from 10 IHPS and 3 controls patients, utilizing specific monoclonal antibody to NCAM(neural cell adhesion molecule). In IHPS patients, the number of NCAM protein immunoreactive nerve fibers were less than that in normal subjects. Auerbach myenteric plexuse was well developed and interbundle nerve plexuse was present but nerve fibers supplying individual muscle cells in smooth muscle bundles were poorly developed. These results indicate reduction of innervation in smooth muscles in IHPS patients that possibly contributes to the pathogenesis of IHPS.
The pyloric length, diameter and muscle thickness were measured by ultrasonograms of 15 infants with infantile hypertrophic pyloric stenosis (IHPS) and were compared with the infants who came in for the routine vaccination randomly. This study analyzed the changes in pylorus for those who received pyloromyotomy using the ultrasonogram at 4 weeks and 8 weeks postoperatively, such as the time needed to become normalized, and compare with the size of the hypertrophic pylorus before the pyloromyotomy. According to Carver5, the pyloric muscle volume (PMV) and pyloric muscle index (PMI) were calculated in each case. The pyloric muscle volume, PMI and the thickness of pyloric muscle proved to be a more reliable guide to diagnose IHPS than length and diameter of pylorus. The pyloric muscle after pyloromyotomy was measured by ultrasound at 4 weeks and 8 weeks postoperatively. The pyloric muscle length, diameter, thickness and pyloric muscle volume were not normalized at 4 and 8 weeks postoperatively. However, pyloric muscle index was normalized at 4 weeks postoperatively which was probably due to rapid weight gain after pyloromyotomy.
Thirty three members of the Korean Association of Pediatric Surgeons were surveyed to determine the clinical manifestations and current management of infantile hypertrophic pyloric stenosis (IHPS). The members completed a registration form and a questionnaire that indicated their treatment preferences for patients treated during 1996. The response rate was 84.8 %, and 23 institutions participated. Three hundred and sixty-three cases of IHPS were analysed. The male to female ratio was 5.15: 1. The presenting symptoms were nonbilious vomiting in 363 cases(lOO %), palpable mass in the upper abdomen in 200 cases (55.1 %) and visible peristaltic waves in 67 cases(l8.5 %). Fluid therapy was done in 161 cases(44.4 %) for preoperative preparation. Twenty patients(5.5 %) were premature. There were 27 low birth weight babies(7.7 %). The onset of symptoms ranged from 1 to 14 weeks of age with a peak occurrence at 2 to 4 weeks of age. Two hundred and thirty-six cases(66.6 %) presented within 4 weeks of age. There was one set of male twins and a family history of twins. The modes of feedings were: breast feeding; 69 cases(24.5 %), formula feeding; 176 cases(62.4 %) and mixed feeding; 37 cases(l3.l %). The preferred diagnostic modalities were ultrasonography (US) 229 cases(63.l %), UGI series 27 cases(7.4 %) and US and UGI series combined 86 cases(23.7 %). Only 21 cases(5.8 %) were operated on without imaging study, ie. with positive physical finding. Perforation of the mucosa during pyloromytomy occurred in 5 cases. All were treated successfully with primary closure. Persistent vomiting over 2 weeks after operation were reported in 5 cases. Three wound infections, one aspiration pneumonia and one postoperative bleeding were reported. There was no mortality in 363 cases.
Citations
Infantile hypertrophic pyloric stensosis(IHPS) occurs in three of 1000 live births, and is a major cause of nonbilious vomiting of early infancy. It's etiology and pathogenesis however are still obscure. The operation of pyloromyotomy described by Ramstedt in 1912 remains the standard treatment. From January 1990 to July 1997, 64 infants with IHPS were treated at the Department of Pediatric Sursery, Yeungnam University Hospital. The ratio of male to female was 7:1, and the most prevalent age ranged from 2 weeks to 8 weeks(81.2%) of age. Fifty-seven infants were first born (57.8percent). The body weight of all patients at admission was below the 50 percentile. Age of onset of symptoms was between 2 and 4weeks of age in 23 cases(35.9 %). All infants had a history of nonbilious vomting, generally projectile in nature. Hypokalemia was noted in 14 cases(21.9%) and hypochloremia in 26 cases(40.6%). In the preoperative ultrasonography, the average muscle thickness, diameter, and length of the pylorus were 6.3 mm, 12.3 mm, and 17.8 mm. A total of 13 associated anomalies were noted in 12 patients. All cases were treated with Fredet-Ramstedt pyloromyotomy. Postoperative wound infection occured in 3 cases. Thirteen cases(20.3%) presented intermittent nonprojectile vomiting after operation. With control of oral intake vomiting subsided within one week in 63 patients, and in thirteen days in another.
Citations
Infantile hypertrophic pyloric stenosis(IHPS) is common in full-term babies, and relatively rare in prematures. The diagnosis of IHPS in premature infants may be obscured because of the lack of classic symptoms and signs and the absence of the standard criteria for ultrasonic diagnosis. The purpose of this study is to discover the clinical differences between premature and full-term infants with pyloric stenosis, and determine the appropriate diagnostic methods for early diagnosis in premature infants. The clinical records of 52 IHPS patients who had been operated upon from October, 1994 to April, 1997 were reviewed. The incidence of IHPS in premature infants was 25 %. The onset of symptom was 4.7 weeks of age in premature, and 2.9 weeks in full-term babies. Diagnosis was established by typical symptoms. signs. and diagnostic imaging studies. In two premature infants, diagnosis was confirmed by upper gastrointestinal(GI) series, because ultrasonography did not meet the diagnostic criteria. Two premature infants initially diagnosed as gastroesophageal reflux by esophagography. were found to have IHPS by upper GI series. For the diagnosis of IHPS, a new set of criteria for premature babies has to be developed.
Citations
Infantile hypertrophic pyloric stenosis is one of the most common disorders requiring surgical therapy during the first few weeks of life. Although the pyloromyotomy, reported by Fredet and Ramstedt, was accepted as a standard procedure of choice, various laparotomy incisions have been reported by several authors. Currently, the most commonly used transverse or right upper quadrant incisions, offer many advantages, but is not without drawbacks. The authors utilized the circumumbilical skin incision and upper subcutaneous dissection followed by vertical division of linea alba in 16 cases of infantile hypertrophic pyloric stenosis. This incision avoids transection of rectus muscle and offers a much better cosmetic result. We prefer this procedure because of acceptable scar and no additional wound complication.
Precocious puberty is difficult to define because of the marked variation in the age at which puberty begins normally, onset of puberty before 8 years of age in girls and 9 years in boys may be considered precocious. The etiology of precocious puberty in boys is usually idiopathic, but can result from adrenal and testicular tumors. The hepatoblastoma that produces hCG is a very rare functioning tumor known to cause precocious puberty in boys. Recently, author experienced one case of virilizing adrenal cortical adenoma in 22 month-old boy, one case of adrenal cortical carcinoma in 28 month-old boy, and one case of virilizing hCG-producing hepatoblastoma in 7 year-old boy and reviewed literatures.
Citations
Citations
 First
First Prev
Prev

